The prognosis for patients with untreated acute aortic dissection is grim, with reported mortality rates greater than 1% per hour during the first day after onset, and as high as 80% at two weeks.
Fortunately, MDCT appears to be up to the task of finding all types of dissections -- if the patient with suspected dissection is lucky enough to get scanned.
A study of patients who underwent MDCT imaging for symptoms suggestive of aortic dissection showed that the modality was highly sensitive and specific for all types of dissection. CT is also faster and generally more accurate than the alternatives, including MRI, ultrasound, and even the invasive gold standard exam, aortography, the authors wrote.
Still, dissection is associated with so many clinical indications, none entirely reliable, that even MDCT yields a positivity rate of less than 20% of patients scanned. Because MDCT makes dissection easier to rule out, however, and because the consequences of missing a diagnosis are so dire, emergency physicians are advised to keep dissection high on the clinical suspicion index until the patient can be cleared.
Researchers have estimated an aortic dissection incidence of 5 million to 127 million people per year, though the true incidence is unknown because as many as a third of cases aren't diagnosed, noted study author Dr. Robert Hayter and colleagues from Massachusetts General Hospital in Boston.
Their study sought to retrospectively review the performance of MDCT for detecting nontrauma aortic dissection in the emergency setting.
"Aortic dissection is associated with several reported risk factors, the most important of which are hypertension and medial degeneration of the aortic wall," Hayter et al wrote in the March issue of Radiology. "Aortic intramural hematoma, a disorder differentiated from aortic dissection by the lack of both a detectable intimomedial flap and direct flow communication between the true and false lumina, has an estimated prevalence of 5% to 20% of all acute aortic disorders identified at presentation. Penetrating aortic ulceration, a disorder associated with increased risk of progression to acute aortic rupture and other acute aortic disorders, has an unknown independent prevalence but has been reported in association with a 2.3% of cases of suspected aortic dissection, and is associated with 52% of aortic intramural hematomas" (Radiology, March 2006, Vol. 238:3 pp. 841-852).
The study examined 365 of 373 patients (204 men and 161 women; mean ages 61 and 69, respectively) suspected of having aortic dissection or other aortic disorders with multidetector-row CT (LightSpeed, GE Healthcare, Chalfont St. Giles, U.K.). The acquisitions consisted of enhanced and nonenhanced chest, abdominal, and pelvic images acquired at 4 x 2.5-mm collimation.
Clinical indications were highly variable and included chest pain in 217 (58.2%), back pain in 162 (43.4%), abdominal pain in 54 (14.5%), syncope in 10 (2.7%), shortness of breath in 21 (5.6%), unequal blood pressure in the arms in five (1.3%), and miscellaneous symptoms in 19 (5.1%) cases, the authors wrote.
"The acquisition of nonenhanced CT images for visualization of the hyperattenuating crescentic hematoma produced by aortic intramural hematomas was followed by the acquisition of contrast-enhanced transverse CT images from the lung apices to the acetabular roof for visualization of the classic intimomedial flap," the group wrote. The second acquisition followed IV administration of 3-4 mL/sec (total 100-120 mL) of iodinated contrast material. In cases that were positive for acute aortic disorder, additional two-minute delay scanning was performed at 4 x 2.5-mm collimation, they noted.
"This examination yielded 7.5-mm contrast-enhanced images with 7.5-mm spacing, which were used to differentiate the initial slow blood flow in the false lumen from the potential free blood flow between the true and false lumina," Hayter and colleagues wrote.
The results showed that 67 (18%) of the 373 cases were interpreted as positive for acute aortic disorder, including 112 acute aortic disorders in the 67 cases: 23 acute aortic dissections, 14 acute aortic intraluminal hematomas, 20 acute penetrating aortic ulcers, 44 new or enlarging aortic aneurysms, and 11 acute aortic ruptures.
Of the 373 cases, 305 (81.8%) were negative for acute aortic disorder, and in 48 of these, MDCT demonstrated alternative findings that accounted for the clinical presentation. Three cases had both aortic dissection and alternative findings and one (0.3%) was indeterminate. In all, 112 findings were found to be positive for acute aortic disorder, an alternative finding, or both.
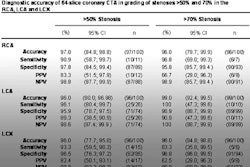
There were 67 true-positive cases and no false positives, for a sensitivity of 99% (67 of 68), specificity of 100% (304 of 304), positive predictive value of 100% (67 of 67), negative predictive value of 99.7% (304 of 305), and accuracy of 99.5% (371 of 373).
In the 373 patients, the positivity rate for suspected acute aortic dissection or other acute aortic disorder was 18%.
"Blood pressure at presentation tended to be normal to high systolic in the acute aortic disorder patients," the team wrote. Among patients with aortic disorder, no systolic blood pressure measurements were 80 mm Hg or lower, one (8%) was 81-99 mm Hg, seven (58%) were 100-139 mm Hg, and four (33%) were 140 mm Hg or higher.
Electrocardiographic findings in acute aortic disorder cases were also variable, but most frequently found in nonspecific ST-T wave interval changes and old Q waves, the authors wrote.
"Nonspecific ST-T wave interval changes were present in 14 (82%) of 17 cases of type A disorder, 17 (53%) of 32 cases of type B disorder, 22 (50%) of 44 cases of new or enlarging aortic aneurysm, and eight (73%) of 11 cases of acute aortic rupture," the authors stated. "Old Q waves were present in three (18%) cases of type A disorder, eight (25%) cases of type B disorder, eight (18%) cases of new or enlarging aortic aneurysm, and three (27%) cases of acute aortic rupture."
Radiologic findings were just as inconsistent in the acute disorder cases. A widened mediastinum was seen in eight (47%) of 17 cases of type A disorder, four (13%) of 32 cases of type B disorder, four (9%) of 44 cases of new or enlarging aortic aneurysm, and seven (64%) of 11 cases of acute aortic rupture.
"Cardiac silhouette enlargement was present in four (24%) cases of type A disorder, seven (22%) cases of type B disorder, six (14%) cases of new or enlarging aortic aneurysm, and three (27%) cases of acute aortic rupture," the group wrote. "Thoracic aortic ectasia was present in three (18%) cases of type A disorder, six (19%) cases of type B disorder, 10 (23%) cases of new or enlarging aortic aneurysm, and three (27%) cases of acute aortic rupture."
Pleural effusion was seen in six (35%) cases of type A disorder, four (13%) cases of type B disorder, 10 (23%) cases of new or enlarging aortic aneurysm, and six (55%) cases of acute aortic rupture, according to the authors. Aortic calcification, displacement of the aorta or mediastinum, and intimal calcification were rare.
Immediate surgical repair, the most common treatment option, was performed in 11 (65%) type A disorders, six (19%) type B disorders, 10 (23%) new or enlarging aortic aneurysms, and 10 (91%) acute aortic ruptures. Two patients with acute aortic ruptures died, while most cases of aortic disorder (82%) were discharged following treatment in stable condition.
"The diagnosis of aortic dissection is now far less complicated and less labor-intensive," the authors wrote. "For primary imaging in cases of suspected acute aortic disorder, aortography has been replaced by CT, MR imaging, or US. These imaging modalities have benefits and limitations, however. CT is readily available in most emergency departments."
MDCT has dramatically increased the speed and accuracy of aortic examination, while MRI's principal drawback is that the exam takes 30 minutes, the authors noted. Ultrasound techniques have also been extensively investigated, and have their own strengths and weaknesses. Transthoracic echocardiography has low sensitivity (60% to 80%) for detecting type A and B dissections, while transesophageal echocardiography (TEE) can raise systolic blood pressure in awake patients, therefore actually increasing the risk of acute aortic rupture.
As a result, MDCT is now the primary imaging modality, except in cases of patient instability, poor renal function, or allergy to iodinated contrast material. In cases of instability, TEE, which can be performed in five minutes, is often a good alternative in these cases.
The 18% positivity rate "provides evidence that the screening of patients in the emergency setting prior to multidetector-row CT is adequate," the authors wrote. "The physician must keep a high clinical index of suspicion for aortic dissection and other aortic disorders in patients in emergency settings because multidetector-row CT can enable a rapid and accurate diagnosis of any acute aortic disorder."
By Eric Barnes
AuntMinnie.com staff writer
March 29, 2006
Related Reading
CT mostly outperforms alternatives in penetrating trauma, February 20, 2006
Medicare to pay for AAA screenings, February 13, 2006
Long-term anticoagulant users show elevated coronary, aortic calcium, December 20, 2005
CT doesn't hurt when evaluating emergency chest pain, August 15, 2005
Copyright © 2006 AuntMinnie.com