A study comparing four exam techniques chose CT and capsule endoscopy (CE) as best of show for diagnosing Crohn's disease in the small bowel. Ileoscopy came in third and has its uses, the authors noted, while the small-bowel follow-through exam showed significant limitations, often producing negative or inconclusive findings.
In reality the best imaging method can depend on the extent and location of the disease, explained Dr. Amy Hara and colleagues from the Mayo Clinic in Scottsdale, AZ, in their report in Radiology. But the strengths and limitations of each method were known at the outset, they wrote.
"Conventional endoscopy, although it provides a direct view of the mucosal surface, is limited to the proximal small bowel or to the distal terminal ileum (in which case it is termed ileoscopy)," Hara, Dr. Jonathan Leighton, Dr. Russell Heigh, and colleagues wrote (Radiology, January 2006, Vol. 238:1, pp. 128-134).
"Ileoscopy is further compromised by the occasional inability to reach the cecum or intubate the ileum during colonoscopy," they noted. "Although barium small-bowel follow-through (SFBT) can effectively depict transmural disease, it may be imprecise for depicting mild disease, such as aphthous ulcers or other subtle mucosal abnormalities."
As for the newer exam techniques, the group wrote: "Capsule endoscopy provides a direct and more extensive mucosal evaluation than standard endoscopy does, whereas CT enterography has the ability to depict subtle findings such as mucosal hypervascularity or mild wall thickening, which are not depicted by standard barium examinations."
In the study, 17 patients with known or suspected nonobstructive Crohn's disease persevered through four exams: CE, CT enterography, colonoscopy with ileoscopy, and SFBT. If the diagnosis or suspicion was based on ileoscopy or SFBT within the previous six months, the exam was repeated, the group noted.
The SBFTs were single-contrast barium exams performed by experienced radiologists using 400-600 mL of barium sulfate suspension. Intermittent palpation and fluoroscopic evaluation was performed every 20-30 minutes until the ileum was visualized.
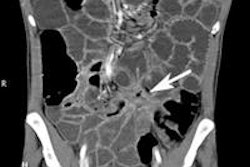
CT enterography was performed after drinking 1500 mL of water at 45 minutes, 30 minutes, and 15 minutes before the procedure. The team began administration of 150 mL nonionic intravenous contrast medium (iohexol, Omnipaque 250, GE Healthcare, Chalfont St. Giles, U.K.) 40 seconds before CT scanning.
Capsule endoscopy (Given Diagnostic System, Given Imaging Systems, Yoqneam, Israel) was preceded by a liquid diet the day before the procedure. After swallowing the capsule with water, patients were allowed to drink water at two hours and permitted to eat solid food at four hours, returning in eight hours to remove the sensor array and data recorder. The video results were interpreted by three experienced board-certified radiologists.
In all, 17 of 20 patients completed all four exams. According to the results, Crohn's disease was depicted by capsule endoscopy in 12 patients (71%), ileoscopy in 11 (65%), CT enterography in nine patients (53%), and SBFT in four patients (24%).
Capsule endoscopy was incomplete in two patients, but had the highest diagnostic yield for Crohn's disease. Ileoscopy was incomplete in four patients and had the lowest diagnostic yield, but the differences were not statistically significant (p = 0.02), the authors wrote. SFBT also missed a stricture in one patient, which resulted in a CE capsule having to be removed surgically. Meanwhile, two extraintestinal findings (mesenteric adenopathy in two patients, perianal and enterocolic fistulas in one patient) were seen by CT and SFBT but not endoscopically.
"This preliminary study demonstrates capsule endoscopy and CT enterography may depict nonobstructive Crohn's disease when techniques such as ileoscopy and SBFT are negative or inconclusive findings," the authors wrote. "SBFT detected far less disease than did capsule endoscopy, CT enterography, or ileoscopy," they wrote. "The suboptimal performance of SBFT in evaluating patients with Crohn's disease compared with ... capsule endoscopy has been observed in other studies."
The small patient cohort was the principal limitation, one that precluded any finding of significance at the 5% level, they noted.
The authors cited a number of possible reasons for SBFT's comparatively poor performance. First, indirect methods of evaluating the small bowel, such as with barium, have a technical disadvantage compared to methods such as endoscopy that can directly visualize the mucosa, they wrote. Also, barium exams that rely on timed overhead radiography are inferior to intermittent fluoroscopy with palpation performed by a radiologist.
"In addition, most studies that involve capsule endoscopy do not include patients with positive barium examination findings or patients with advanced disease and strictures and obstruction," the authors explained. "The reasonable conclusion from most studies is that capsule endoscopic findings are often positive in patients with negative barium examination findings, not that barium examinations are inadequate for depicting small-bowel disease." CE can also be compromised by poor bowel prep, and the capsule may not reach the cecum, they wrote.
The study had only one patient with fistulas, detected by both SBFT and CT. But the authors noted that other studies have found that CT is superior to SBFT for detecting extraluminal findings and complications of Crohn's disease, and in fact, CT altered the management of nearly a third of the patients in these studies.
The argument also could be made that if CT enteroclysis techniques rather than CT enterography had been used, more Crohn's disease would have been detected, but, in any case, studies have shown that CE depicts small-bowel ulcers that cannot be detected by radiologic imaging, they wrote, and is better for assessing proximal or early mucosal disease.
Ileoscopy, which performed comparably to CE in the study, is still a useful technique for evaluating inflammatory bowel techniques, the group wrote, although its inability to demonstrate mucosa proximal to the distal ileum can produce false-negative diagnoses.
"In our study, two patients with proximal and middle small-bowel ulcers and erosions at CE had negative findings at ileoscopy," they wrote. "Therefore, while ileoscopy can successfully depict Crohn's disease, capsule endoscopy or CT enterography still can play an important role, particularly for depicting proximal disease or for patients in whom the ileoscopy examination was incomplete."
By Eric Barnes
AuntMinnie.com staff writer
January 25, 2006
Related Reading
CT differentiates mesenteric ischemia from transmural necrosis, January 3, 2006
Success begets growing role for CT enteroclysis, November 18, 2004
Capsule endoscopy best in spotting small bowel cause of obscure GI bleeding, December 12, 2005
Survey finds most small-bowel exams are substandard, April 16, 2004
Capsule endoscopy fares well in small bowel versus CT, barium enema, January 14, 2004
Copyright © 2006 AuntMinnie.com