Researchers in Korea have found CT useful for differentiating transmural ischemic necrosis from nontransmural ischemia, potentially sparing some patients the need for surgical intervention.
Mesenteric venous thrombosis is an uncommon but potentially deadly cause of mesenteric ischemia, said Dr. Seung Soo Lee at the 2005 RSNA meeting in Chicago.
Clinical features of acute bowel ischemia include pain, nausea, and vomiting, and constipation with or without bloody diarrhea.
Management of gastrointestinal bleeding has changed in recent years, Lee said. "In the past, surgical exploration and resection of the affected bowel was the mainstay of treatment," he said. In recent years, however, anticoagulation therapy has become the frontline therapy, and "subsequent treatment is now dependent on the severity of bowel ischemia. Therefore, assessment of bowel viability is important in management of patients with venous thrombosis," he said.
To assess whether CT features could distinguish transmural ischemic necrosis from nontransmural ischemia, the researchers from the University of Ulsan College of Medicine and the Asan Medical Center in Ulsan, South Korea, analyzed CT data from 22 patients retrospectively.
"We included 27 patients (mean age 55) with symptomatic mesentery ischemia secondary to acute mesentery venous thrombosis," Lee said. They were examined with single-slice (n = 14) or four- or 16-slice multidetector-row CT (n = 13), following administration of 100-150 mL of contrast material at 2.5-3 mL per second and a scan delay of 72 seconds.
Thirteen of the patients underwent small bowel resection and were diagnosed with transmural ischemic necrosis. Of the remaining group, 12 patients responded to anticoagulation therapy, and were considered to have reversible ischemia based on the clinical and CT follow-up, and the remaining two patients underwent small bowel resection and were found to have transmural ischemia.
The CT scans were evaluated for the location of venous thrombus, degree of bowel wall thickening and enhancement, presence of bowel dilatation, amount of ascites, and extent of mesenteric haziness. The researchers compared CT findings between the patients with transmural ischemic necrosis and reversible ischemia.
"All CT images were prospectively evaluated by consensus of two radiologists, who graded the severity of bowel ischemia ... and the severity of thrombosis," Lee said.
The sensitivity, specificity, and positive predictive value of CT findings for the diagnosis of transmural ischemia were decreased bowel wall enhancement, 91.8%, 90.9%, and 90%; large amount of ascites, 90.9%, 63.6%, and 71.4%; and diffuse mesenteric haziness, 81.8%, 63.6%, and 69.2%, respectively, the authors wrote in their abstract.
Other CT findings, including location of venous thrombus (p = 0.097), degree of bowel wall thickening (p = 0.7), and the presence of bowel dilatation (p = 0.28), did not show a statistically significant difference.
Venous thrombus was present in all the patients. All patients also showed bowel wall thickening with mean thickness of 9.5 ± 3.2 mm (range of 5-17 mm). Decreased bowel wall enhancement (p = 0.001), large amount of ascites (p = 0.027), and diffuse mesenteric haziness (p = 0.24) were more frequently found in patients with transmural necrosis than those with reversible ischemia.
"Bowel segments with homogenous enhancement or decreased enhancement were (more common) in patients with transmural infarction," Lee said. "Bowel segments with layered enhancement were significantly more common in patients with nontransmural ischemia, and the difference in lumen diameter was statistically significant between the two groups. Lumen diameter greater than or equal to 20 mm was mostly seen in patients with transmural infarction; lumen diameter less than or equal to 10 mm was only seen in patients with nontransmural ischemia. There was no statistically significant difference in bowel thickness or the extent of thrombosis.... A large amount of ascites was only seen in patients with transmural infarction."
Multifactorial logistic regression analysis showed bowel segments with decreased enhancement and lumen narrowing were two independent significant variables that differentiated transmural infarction from nontransmural ischemia, he said.
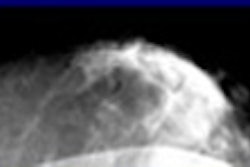
In a 31-year-old man with nontransmural ischemia, CT showed thrombosis and wall thickening of the jejunum in a layered enhancement pattern and a comparatively high degree of enhancement in the ischemic jejunum, which had a lumen diameter less than 10 mm.
"This patient underwent small bowel resection, and ... there was no evidence of transmural infarction," Lee said.
And in the case of a 43-year-old man with nontransmural ischemia, CT showed thrombosis, wall thickening in the jejunum, and a layered enhancement pattern that was higher in the ischemic jejunum. The patient was treated nonsurgically and released, he said.
"Increased bowel wall thickness or decreased homogeneity of enhancement, a large amount of ascites, diffuse mesenteric haziness, and distended bowel lumen are -- along with segments with decreased enhancement and lumen diameter -- independent factors that could differentiate transmural infarction from nontransmural ischemia," Lee said.
Thus in patients with acute mesenteric venous thrombosis, CT can be of value in diagnosing as well as differentiating transmural infarction from nontransmural ischemia, Lee concluded. The main contribution of MDCT over single-slice CT has been the identification of smaller infarcts, he added.
By Eric Barnes
AuntMinnie.com staff writer
January 3, 2006
Related Reading
Urgent colonoscopy not seen to improve outcomes after lower GI bleed, December 20, 2005
Capsule endoscopy best in spotting small bowel cause of obscure GI bleeding, December 12, 2005
Success begets growing role for CT enteroclysis, November 18, 2004
Survey finds most small-bowel exams are substandard, April 16, 2004
Capsule endoscopy fares well in small bowel versus CT, barium enema, January 14, 2004
Copyright © 2006 AuntMinnie.com