Venous air embolization:
Clinical:
Click here for discussion of "Systemic" air embolism following percutaneous biopsy
Venous air embolism can occur as a complication of thoracic trauma, surgery, or rarely following percutaneous lung biopsy. In humans, the lethal volume of intravenous air is usually between 300 and 500 ml injected at a rate of 100 ml/sec [2]. However, injection of as little as 100 ml's can result in death [2]. The major effect of venous air embolism is to obstruct the right ventricular pulmonary outflow tract. Typically patients experience the sudden onset of air hunger, dyspnea, cough, dizziness, and chest pain. Tachycardia, tachypnea, and hypotension are noted on physical exam. Neurologic symptoms such as altered mental status, convulsions, and coma occur in 42% of patients. Treatment is directed as restoring cardiopulmonary circulation and promoting reabsorption of the intravenous air. The patient should be placed in a left lateral decubitus head down position because it causes right-sided cardiac air to rise to the periphery of the right atrium [2]. Ventilatory support with 100% oxygen should be administered to promote resorption of air bubbles [1,2].
X-ray:
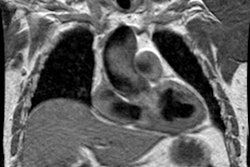
The CXR is usually normal. Air in the distal pulmonary artery may appear in a characteristic bell shape.
REFERENCES:
(1) J Thorac Imag 1997; Klein JS, et al. Transthoracic needle biopsy: An overview. 12: 232-249
(2) AJR 2000; Rossi SE, et al. Nonthrombotic pulmonary emboli. 174: 1499-1508