Fibrosing Mediastinitis:
(Click on small images to view the larger radiograph)
The patient was in his mid-twenties with a history of Histoplasmosis infection. The patient had done well despite the presence of persistent mediastinal adenopathy, but had recently begun to experience episodes of hemoptysis.
The frontal chest radiograph demonstrated right paratracheal and right hilar fullness.
A patchy opacification can be seen in the right upper lobe- best appreciated in the
retrosternal clear space on the lateral view.


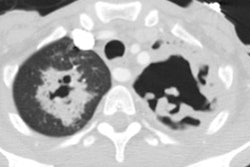
A series of computed tomography images of the chest revealed the presence of calcified adenopathy in the right suprahilar/lower right paratracheal and subcarinal regions (red arrows on the non-contrast examination). Following the adminsitration of I.V. contrast, the vascular structures in the right suprahilar region appear compressed. The lung windows demonstrate attenuation of the right upper lobe pulmonary vein (red arrows) in comparison to the left side (blue arrows). Additionally, multiple areas of peripheral consolidation are evident.
A pulmonary arteriogram revealed a normal appearing take-off of the right upper lobe
pulmonary artery, but there was severe pruning of the peripheral right upper lobe
pulmonary arteries and markedly diminished capillary blush.
At bronchoscopy blood was evident in the right upper lobe airways. The findings were felt to be consistent with fibrosing mediastinitis with compression/obliteration of the right upper lobe pulmonary vein, with resultant venous infarction (producing areas of consolidaiton), and secondary pulmonary artery hypertension due to the venous obstruction (as reported by Dye et al. in The Journal of Thoracic and Cardiovascular Surgery 1977; Sclerosing mediastinitis with occlusion of pulmonary veins. 74 (1): 137-141)