When healthcare practitioners think of computer-aided detection (CAD) technology today, they usually consider using it with mammography for early breast cancer detection. As technology and research progress, however, there is a developing consensus among radiologists that CAD can aid in uncovering abnormalities in applications such as breast MRI, lung cancer screening, and virtual colonoscopy exams.
CAD, for example, is helping radiologists more accurately determine the size and location of cancers found with breast MRI. A study released in May from the Clinica Girona in Girona, Spain, compared CAD to breast imaging software that comes standard on MRI systems.
Dr. Joan C. Vilanova, Clinica Girona MR department director and lead author of the study, reported that the quality of the final postprocessed CAD images was better than images derived from standard breast MRI visualization software in 83% of the cases. It also took radiologists an average of 12 minutes to analyze and interpret an image with CAD (CADstream, Confirma, Kirkland, WA), compared with 19 minutes for the standard MRI software images.
Both systems detected additional lesions in 10 patients, eight of whom were scheduled to undergo a lumpectomy prior to the MRI examination. Their treatment was changed to a mastectomy after the additional review. The cancerous lesions would have remained in the breast had the breast MRI not been performed, Vilanova said.
Image volume crunch
With breast MRI, the number of images per exam easily can exceed 2,000, "which is a tremendous amount of data to try to process in any type of expedient fashion," noted Dr. Andrew Osiason, director of abdominal imaging for New Century Imaging in Oradell, NJ.
"If you're looking to streamline workflow, as well as improve accuracy and standardize reports for breast MR, you have to have a CAD system in place," he said.
New Century's radiologists handle 30 to 40 breast MR cases per week from their primary imaging facility, outpatient practices, and Hackensack University Medical Center in Hackensack, NJ. For the past two years, the imaging center has used breast MR CAD software (CADstream, Confirma) that automatically processes MR studies on a networked server and delivers datasets for viewing on New Century's PACS.
Osiason said the key characteristic with breast MRI CAD is its functionality.
"You're able to customize hanging protocols, instantaneously look at (contrast) curve kinetics -- which is one indicator whether a lesion may be benign or malignant -- lesion morphology, and pulse sequences in a quick manner," he said.
A soon-to-be released CADstream upgrade will add additional functionality, including a multimodality configuration to access, view, and reference patients' mammography and ultrasound studies, while interpreting breast MR, Osiason said.
"Clearly, breast MRI needs to be looked at in conjunction with mammography or breast ultrasound," he added. "To have all of that on one system is very beneficial."
While breast MR exams in most practices have been "growing at an exponential rate," that growth is not dependent on CAD, Osiason said.
"The question is, 'How would we keep up with that growth?'" he said. "And CAD enables us to keep up with rising volume of breast MR in our practice."
 |
| CAD volume summary of a breast MR image. Image courtesy of Seattle Cancer Care Alliance and Confirma. |
In other breast MR CAD product developments, Alan Penn & Associates of Rockville, MD, is working on what it describes as an adjunct to breast CAD designed to help radiologists differentiate between benign and malignant tumors. In its abstract presented at the 2004 RSNA meeting in Chicago, the company describes CADimas as a system that analyzes 1D, 2D, and 3D data "provided by dynamic T1-weighted breast MR images, and identifies suspicious texture, morphologic and kinetic attributes of enhancing focal masses."
Development of CADimas is fueled by $3 million in Small Business Innovative Research (SBIR) grants from the National Institutes of Health. CADimas currently is in the final year of a three-year study of breast MR images taken from MR scanners from GE Healthcare, Philips Medical Systems, and Siemens Medical Solutions, using various protocols. The study is set to conclude in February 2006.
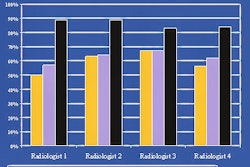
The most recent results were presented in May at the International Society for Magnetic Resonance in Medicine (ISMRM) meeting. The study asked 35 radiologists from around the U.S. to interpret images, and a month later gave them the images to read a second time with computer support, resulting in what CADimas president Alan Penn, Ph.D., described as "statistically significant improvement" in the interpretations. Still, Penn said, there is room for improvement.
"We found that the readers were good at evaluating morphological shape and the basic area of how extensive the lesion was," he said. "Evaluating the margins and evaluating background texture (the radiologists) were not particularly good at."
 |
| Morphological map generated by CADimas of invasive lobular breast carcinoma. Lesion is tagged as being highly suspicious. Image courtesy of Penn & Associates. |
Penn, a mathematician from George Washington University (GWU) turned CAD developer, attributed the discrepancy to the fact that "the mathematical patterns are so subtle that it is virtually impossible for the mind to absorb all the data. It just can't pick up variations along the border or in the border that the computer can."
Penn expects to submit CADimas for FDA clearance before next February, with market availability in 2006.
CAD's influence
Dr. Rachel F. Brem, director of the Breast Imaging and Interventional Center at GWU Medical Center, is one of the specialists evaluating Penn's technology. She also was the principal investigator on the clinical trials that resulted in FDA clearance for iCAD's Second Look CAD product for mammography.
CAD is used in every screening and diagnostic mammogram at GWU -- approximately 80 cases per day -- including images from the center's mobile mammography outreach program in the local community.
"I wouldn't even consider reading a screening board without CAD, because it makes it a much easier process," Brem said. "It is so good at detecting calcifications that I rely on it enormously to help find the clusters of calcifications."
 |
| CAD algorithm marks regions for physicians to zoom in on. Image courtesy of iCAD. |
With more healthcare providers transitioning from analog film mammography to full-field digital mammography (FFDM), Brem said that reading images becomes "seamless" with software producing the CAD-enhanced images on a workstation monitor, adding no additional time to the workflow.
"It is irrelevant in terms of time addition for inspecting images with CAD, as opposed to without CAD," she said.
Brem says the one-time barrier to breast CAD implementation -- reimbursement -- is not an issue anymore in mammography, as more third-party payors and insurance companies see CAD as a medical necessity in patient evaluations. Reimbursement for mammography CAD varies by region and payor, with Medicare reimbursement ranging from $20 to $35.
CAD received two strong endorsements from insurers in recent months. In April, Aetna issued a bulletin saying that it "considers computer-aided detection (CAD) a medically necessary adjunct to mammography." CIGNA announced in November 2004 that it reviewed its existing policy on CAD and determined that CAD had become a standard of care for larger radiology practices.
The companies' declarations are important for two reasons: reimbursement and malpractice litigation.
"We may well find that the question of whether computer-aided detection was employed or not could become a consideration in whether appropriate care was provided to a patient," said iCAD president and CEO Scott Parr. "That's the wrong way to get to that result, but it is unfortunately a likely one."
Practitioners should "realize that CAD will improve patients' outcomes that are so much their concern, and the economics today of CAD tend to provide support for offering that service without putting a small or large practice at a financial disadvantage," he said.
By Wayne Forrest
AuntMinnie.com contributing writer
July 13, 2005
"Part II: Computer-aided detection marking new targets" will examine reimbursement and workflow issues for CAD, as well as the technology's burgeoning role in multislice CT and virtual colonoscopy.
Related Reading
VC CAD shows progress toward clinical use, June 3, 2005
CAD struggles through tagged, subtracted VC data, May 18, 2005
Support vector machines boost accuracy of VC CAD, May 3, 2005
CAD segmentation for mammo acceptable – except in heterogeneously dense breasts, April 26, 2005
CAD offers promising second opinion, even in dense breasts, March 15, 2005
Copyright © 2005 AuntMinnie.com