AJR Am J Roentgenol 1997 Jun;168(6):1541-1548. Pulmonary mucormycosis: radiologic findings in 32 cases.
McAdams HP, Rosado de Christenson M, Strollo DC, Patz EF Jr
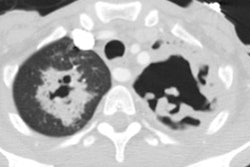
OBJECTIVE: The purpose of this study was to characterize the radiologic manifestations of pulmonary mucormycosis with clinical and pathologic correlation. MATERIALS AND METHODS: Clinical records, pathology reports, chest radiographs, and CT scans of 32 cases of pathologically proven pulmonary mucormycosis were retrospectively reviewed. RESULTS: The study group included 20 males and 12 females with a mean age of 47 years old. Clinical data were available for 29 patients. Signs and symptoms included fever (n = 23), cough (n = 21), bloody sputum (n = 9), dyspnea (n = 7), and chest pain (n = 6). Four patients were asymptomatic. Most patients were either immunocompromised (n = 20) or had diabetes mellitus (n = 9). Sputum or bronchoalveolar lavage cultures showed no growth in 17 of 18 cases. Diagnoses were confirmed at surgery or autopsy in all cases. Abnormalities seen on chest radiographs included lobar (n = 15) or multilobar (n = 6) consolidation, solitary (n = 7) or multiple (n = 1) masses, and solitary (n = 3) or multiple (n = 2) nodules. Cavitation was seen on chest radiographs in 13 patients, and intracavitary masses were seen in four. Associated radiographic findings included hilar (n = 3) or mediastinal (n = 3) adenopathy and unilateral (n = 6) or bilateral (n = 3) pleural effusion. CT in 19 patients revealed these significant additional findings: splenic (n = 1) or renal (n = 1) involvement, bronchial occlusion (n = 1), extrapulmonary invasion (n = 1), and pulmonary artery pseudoaneurysm (n = 1). CONCLUSION: In our study, pulmonary mucormycosis typically was manifested in immunocompromised or diabetic patients by consolidation on chest radiographs; cavitation was seen in 40% of patients. CT revealed significant unsuspected abnormalities in 26% of patients. Definitive diagnosis required pathologic demonstration of the organism in affected tissue because cultures from our patients rarely showed growth.
PMID: 9168721, MUID: 97312280