MRI-guided focused ultrasound (MRgFUS) therapy can successfully treat prostate cancer for those at intermediate risk, a study published March 5 in Radiology found.
Researchers led by Sangeet Ghai, MD, from the University of Toronto in Canada found that MRgFUS led to no adverse effects and negative follow-up results two years after treatment.
“Additionally, there was no significant decline in quality of life per the validated questionnaires,” Ghai and colleagues wrote.
MRgFUS allows for clinicians and interventional radiologists to accurately target localized areas deemed to be clinically significant, including for treating prostate cancer. Previous research also highlights that this method can preserve more healthy tissue. However, Ghai and co-authors noted that the long-term outcomes of MRgFUS in prostate cancer treatment are not well known.
In a single-center study, the team assessed the two-year oncological and functional outcomes of men with intermediate-risk prostate cancer. Study participants underwent transrectal MRgFUS between 2016 and 2019. The team noted that planned ablation volumes included 10-mm margins when possible.
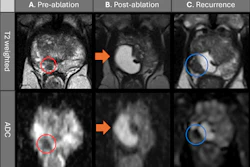
 Images depict biopsy-confirmed prostate cancer in a 56-year-old man. (A) Pretreatment axial T2-weighted fast spin-echo MRI scan and (B) apparent diffusion coefficient map acquired with a 3T scanner show the tumor in the left transition zone (arrows). (C) Intraoperative 1.5-T MRI scan shows the contoured rectal wall (red line), prostate margin (blue outline), and region of interest (orange outline). (D) Intraoperative MRI scan shows a focused ultrasound beam path (blue) overlaid on the treatment plan. The rectangular boxes show each sonication spot. (E) Thermal map obtained during treatment shows heat deposition color-coded in red and overlaid on the sonication spot. (F) Axial gadobutrol-enhanced MRI scan obtained immediately after treatment shows the devascularized ablated volume (arrows). (G) Corresponding T2-weighted fast spin-echo 3T MRI scan obtained at 24 months after ablation shows fibrosis and volume loss in the left transition zone (arrows). Findings from a biopsy showed scar tissue, negative for malignancy at the treatment site.RSNA
Images depict biopsy-confirmed prostate cancer in a 56-year-old man. (A) Pretreatment axial T2-weighted fast spin-echo MRI scan and (B) apparent diffusion coefficient map acquired with a 3T scanner show the tumor in the left transition zone (arrows). (C) Intraoperative 1.5-T MRI scan shows the contoured rectal wall (red line), prostate margin (blue outline), and region of interest (orange outline). (D) Intraoperative MRI scan shows a focused ultrasound beam path (blue) overlaid on the treatment plan. The rectangular boxes show each sonication spot. (E) Thermal map obtained during treatment shows heat deposition color-coded in red and overlaid on the sonication spot. (F) Axial gadobutrol-enhanced MRI scan obtained immediately after treatment shows the devascularized ablated volume (arrows). (G) Corresponding T2-weighted fast spin-echo 3T MRI scan obtained at 24 months after ablation shows fibrosis and volume loss in the left transition zone (arrows). Findings from a biopsy showed scar tissue, negative for malignancy at the treatment site.RSNA
The study participants also completed quality-of-life questionnaires at six weeks and at five, 12, 18, and 24 months. Additionally, the team collected data regarding adverse events. To confirm their findings, the researchers at 24 months performed multiparametric MRI as well as targeted and systematic biopsies.
The study included 44 men with a median age of 67 years. Of the total, 36 study participants had a grade group of 2, and eight had a grade group of 3. Both grade groups indicate intermediate risk to the point where therapies should be used.
The researchers highlighted the success of MRgFUS in the patients, reporting that treatment was successfully completed in all participants and no major adverse events were recorded. One participant refused biopsy at 24 months.
Two years following treatment, 39 of the remaining 43 participants (91%) had no clinically significant prostate cancer at the treatment site and 36 participants (84%) had no cancer in the entire gland.
Finally, the team reported no changes in International Index of Erectile Function-15 score or International Prostate Symptom Score during the two-year follow-up (p = 0.73 and 0.39, respectively). This indicates that the patients experienced no significant decline in quality of life following MRgFUS treatment.
The study authors highlighted that their results could help in widespread adoption of MRgFUS in appropriately selected patients.
In an accompanying editorial, David Woodrum, MD, PhD, from the Mayo Clinic in Rochester, MN praised the study as having “excellent local control, lack of substantial development of cancer elsewhere in the prostate, and no change in urinary or erectile function.”
“The study…reinforces the concept that accurate ablation monitoring can keep morbidity low and cancer control high,” Woodrum wrote. “Overall, this study is an excellent representation of the possibilities of treatment expansion in patients with prostate cancer.”
The full study can be found here.