Wednesday, December 2 | 9:00 a.m.-9:10 a.m. | VI41-02 | Room E352
Recent research has determined that inflamed plaque is at the highest risk for rupture and causing stroke. Could ultrasound of the carotid artery be used as a tool to detect which patients have inflamed plaque, enabling therapeutic intervention?U.K. researchers tested this theory in a group of 29 patients, eight of whom were symptomatic for carotid stenosis > 50%, while 21 were asymptomatic. They used a microbubble contrast agent commercially available in Europe (SonoVue, Bracco Imaging, Milan, Italy) and scanned patients with an iU22 system with an L12-5 probe (Philips Healthcare, Andover, MA).
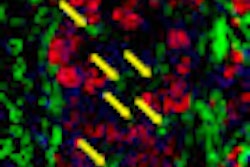
The researchers performed late-phase flash imaging at an intermediate mechanical index six minutes after injection of the contrast bolus. Software was used to quantify the degree of contrast accumulation in carotid plaque, and signal intensity between symptomatic and asymptomatic patients was compared, according to presenter Dr. David Owen of Imperial College of London.
During the dynamic phase, the researchers found that signal from the lumen is three orders of magnitude greater than signal from plaque. But during the late phase, after most of the contrast has been cleared from the vascular space, the two signals are of equal magnitude. This implies that late-phase imaging is visualizing contrast adhering to inflamed plaque, and not contrast perfusing the plaque.
The researchers found that the late-phase signal intensity was much higher for the symptomatic group compared to the asymptomatic patients, although there was a subset of asymptomatic patients whose plaque values overlapped the symptomatic patients.
"We have been able to demonstrate that patients with recent stroke (i.e., those whose plaques are highly likely to be inflamed) have much greater signal than those who have never had a stroke (i.e., those whose plaques are not likely to be inflamed)," Owen said. "The implication, if this painless and quick imaging test proves to be successful, is that those who are at risk of stroke can be identified and therefore undergo preventative surgery."
The researchers recommended that a study be conducted comparing late-phase contrast-enhanced ultrasound to histology to confirm that contrast ultrasound is indeed detecting inflammation.