Dear Digital X-Ray Insider,
Converting to digital x-ray is a necessary step for any modern imaging facility. But digital x-ray's inevitability doesn't mean it's without its challenges.
We deal with several of those challenges today in your Digital X-Ray Insider. First up is an article on computed radiography (CR) exposure creep -- the phenomenon in which facilities that convert to CR gradually see radiation dose rise as radiologic technologists use higher exposure settings.
Exposure creep occurs because CR image quality isn't degraded by overexposure, and higher exposure settings usually produce better image quality. Sites using CR need to implement active quality assurance programs to counter the phenomenon; how to do this is the subject of this edition's Insider Exclusive -- an article you're reading before the rest of the AuntMinnie.com membership.
On the other side of the coin, digital radiography (DR) can produce artifacts of its own. Another article we're highlighting this week details how to recognize some of those artifacts, and what you can do to correct for them. You'll find that article by clicking here.
In other news in the Digital X-Ray Community in the past few weeks:
- The U.S. government has proposed a revision to its program for screening coal miners for lung disease that will (finally) allow digital x-ray to be used in addition to film-based systems.
- In a related story, U.S. researchers found that CR is at least equivalent to analog radiography for recognizing small pulmonary opacities from pneumoconiosis.
- Researchers from Massachusetts General Hospital found that an iPad can be used for assessing pneumothorax on plain radiography films.
- Federal investigators found evidence of "questionable" billing practices in portable x-ray services paid for by Medicare.
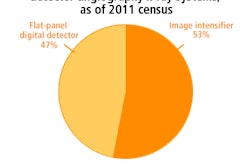
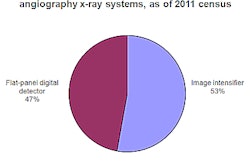
- Procedure-volume growth has stalled at interventional radiology labs using conventional angiography equipment, according to a recent market research report.
Finally, check out our two-part series covering the symposium on medical radiation dose last month in Washington, DC. While much of the discussion pertained to CT, any efforts to better track radiation dose could also involve radiography. Click here for part 1 of the series on the challenges of dose tracking, and click here for part 2 on the uncertainty in calculating medical radiation risk.