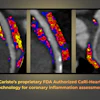
Augmented reality-guided localization successfully replaces CT-guided localization for early-stage lung cancer sublobar resection, achieving noninferiority while reducing radiation exposure, preoperative pain, and procedure time in a single operating room encounter.
- AR-guided approach achieved 98.5% success rate for sublobar resection, meeting noninferiority compared to CT's 99.3% success rate
- Radiation exposure reduced from 1,260 mGy to 456 mGy with AR guidance, representing a 64% reduction
- Preoperative pain scores dropped from 5 to 0 with AR-guided localization versus CT guidance
- Puncture time decreased from 6.5 minutes to 0.6 minutes, and localization-to-incision interval reduced from 33.5 to 2.0 minutes
Augmented reality (AR)-guided percutaneous localization could achieve successful sublobar resection in early-stage lung cancer patients, suggest findings published July 8 in JAMA Surgery.
Single-encounter AR-guided localization achieved noninferiority when compared to CT-guided localization for achieving successful sublobar resection and led to improved patient experience, wrote a team led by Zuodong Song, MD, from Shanghai Jiao Tong University in China.
“This efficient approach may support broader adoption and clinical translation of AI-enabled digital-twin AR platforms,” the Song team wrote.
Preoperative localization is often used to achieve successful sublobar resection with adequate margins for suspicious pulmonary nodules found on CT. However, conventional CT-guided localization has its share of drawbacks. The researchers noted that this involves a multiple-encounter workflow that may cause pain, radiation exposure, and complications for patients.
Song and colleagues developed an AR-guided localization technique using a patient-specific digital-twin model using preoperative end-inspiratory CT images holding anatomical and nodule information.
“AR integrates digital content with the real-world environment in real time,” they highlighted. “By fusing the digital twin with the surgical field via an AR headset, this technique provides CT-free guidance. This enables a single-encounter procedure in which localization and resection are performed in the operating room under general anesthesia.”
The researchers compared the performance of this approach to that of conventional CT-guided percutaneous localization in a multicenter randomized clinical trial.
Final analysis included 270 patients from five medical centers; this included 134 patients in the AR cohort and 136 in the conventional cohort.
The AR-guided approach achieved noninferiority compared to CT guidance for successful sublobar resection. It also led to lower radiation exposure, lower preoperative pain, shorter puncture time, and shorter localization-to-incision interval.
Performance of AR-guided, CT-guided localization | |||
Measure | CT guidance | AR guidance | P value |
Sublobar resection success rate | 99.3% | 98.5% | < 0.001 (for noninferiority) |
Localization error | 3.0 mm | 3.0 mm | 0.08 |
Median radiation exposure | 1,260 mGy | 456 mGy | < 0.001 |
Preoperative pain | 5 | 0 | < 0.001 |
Puncture time | 6.5 | 0.6 | < 0.001 |
Localization-to-incision interval | 33.5 | 2.0 | < 0.001 |
Finally, pneumothorax occurred in 40 of 136 CT-guided cases, the researchers found.
The study authors wrote that centers need thin-slice preoperative CT, 3D reconstruction capability, an AR headset with software, and a reliable registration workflow to implement the AR approach. Operator training in AR workflow and puncture will also be needed, they added.
And while the team did not study cost-effectiveness in its study, it noted that AR adoption “may vary across settings because of equipment, integration, and training costs.”
“In our study setting, digital-twin reconstruction was incorporated into routine workflow without additional charge, whereas the CT-guided pathway involved CT scanner use and patient transfer, which may represent resource utilization,” the authors wrote. “These economic implications should be evaluated prospectively in future multicenter studies.”
Future trials should consider "more robust" comparators beyond traditional CT-guided approaches, according to an accompanying editorial written by Smita Sihag, MD, from the Memorial Sloan Kettering Cancer Center in New York.
Sihag, however, noted that approaches such as the one studied by Song and colleagues could "represent a paradigm shift in thoracic surgery."
"The concept of a on-stop workflow—where diagnosis, localization, and therapeutic resection occur in a single anesthetic—aligns with where the field is heading and the broader push toward integrated, patient-centered care pathways," Sihag wrote.
Read the full study here.