Quantitative computer-aided analysis of chest CT (QCT) scans can help clinicians predict COVID-19 outcomes in hospitalized patients by providing information on a new metric: compromised lung volume, according to a preprint article published May 23 on Research Square, a platform for sharing manuscripts ahead of peer review.
The findings could help doctors better triage patients during the pandemic, wrote a group led by Dr. Ezio Lanza of the Humanitas Clinical and Research Center in Milan.
"The compromised lung volume [measure] is accurate in predicting the need for oxygenation support and intubation and is a significant risk factor for in-hospital death," the group wrote. "QCT may serve as a tool for the triaging process of COVID-19."
In March, Italy -- particularly the Lombardy area -- was a COVID-19 epicenter, and the area's healthcare system was impacted by the patient surge, manifested particularly in a shortage of intensive care beds and ventilators, the group wrote. Some consider CT to be the most sensitive imaging modality for diagnosing COVID-19, but its specificity can be limited -- which is why using computer-aided quantitative analysis with CT could be helpful.
"In our institution, most patients received chest CT at admission, only interpreted visually," the group noted. "Given the proven value of QCT in the setting of ARDS [acute respiratory distress syndrome], we tested QCT as an outcome predictor for COVID-19."
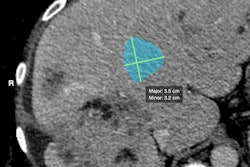
Lanza's group conducted a study that included 222 patients hospitalized between January 25 and April 28 who underwent chest CT on admission due to respiratory symptoms. The researchers characterized each patient's lung volumes and reviewed clinical data such as how much oxygen support patients required during their hospital stay. The investigators then used a computer algorithm to analyze the CT images, assessing its performance using the area under the receiver operating characteristic curve (AUC) measure.
Of the 222 patients, 75% received oxygen during hospitalization (intubation rate: 20%). Lanza and colleagues found that patients with compromised lung volumes in the 6% to 23% range were at increased risk of requiring oxygenation, and those with compromised lung volumes above 23% were at risk for intubation.
The quantitative CT algorithm accurately predicted patients' need for oxygen support or intubation.
| Quantitative CT algorithm's predictive performance in hospitalized COVID-19 patients | |
| Factor | AUC |
| Need for oxygenation support | 86.9 |
| Need for intubation | 89.88 |
| Outcome of oxygenation support | 0.83 |
| Intubation outcome | 0.86 |
The team also found that higher compromised lung volumes also proved to be a risk factor for patient death, with a hazard ratio of 1.02.
QCT shows promise as a tool that can help clinicians determine which patients will soon be in need of a ventilator and which patients may no longer need one, according to Lanza and colleagues.
"[Chest CT's] value is currently limited to visual findings, whereas QCT proved to be a tool that allowed for considerable advancements in understanding ARDS pathophysiology and establishing adequate oxygenation support," they concluded.