VIENNA - The first results of a sizeable Italian multicenter screening trial suggest once again that CT screening of smokers is effective in finding lung cancer in time to cure it.
The results, which compare favorably to earlier data in similar populations, are among the first of several randomized trials undertaken to assess the efficacy of CT lung cancer screening. The research is aimed, in part, at determining whether the results of the nonrandomized International Early Lung Cancer Action Program (I-ELCAP) trial by Henschke et al, which strongly suggested a mortality benefit in more than 30,000 patients, can be replicated in a randomized cohort.
On opening day of the 2007 European Congress of Radiology (ECR), Dr. Giulia Picozzi from the University of Florence presented the baseline scan results of more than 3,000 heavy smokers recruited at four centers in Italy's Tuscany region and who were referred with the help of medical practitioners.
"The aim of our study was to evaluate a possible reduction of mortality with low-dose annual screening with CT, hopefully by including data from other ongoing trials," she said.
In all, 1,406 subjects in the active arm underwent the annual low-dose screening exams. The control arm, nearly identical in "sex and age and smoking habits," underwent no screening.
In the screening group, the researchers "performed follow-up immediately when there was a high suspicion of malignancy," Picozzi said. Subjects with solid nodules 3.5 mm or larger, or nonsolid nodules 5 mm or larger, at baseline scanning underwent CT follow-up at three months. Those with part-solid nodules of any size at baseline were also followed up at three months, reflecting their higher risk of malignancy. PET/CT was reserved for individuals with nodules 7 mm or larger.
"If PET/CT was positive, (CT-guided) fine-needle aspiration (FNAC) was performed; if PET was negative, we scheduled a follow-up," Picozzi said.
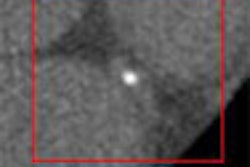
The results showed 405 individuals had noncalcified solid nodules larger than 5 mm in diameter or pure ground glass opacities larger than 1 cm or part-solid nodules.
In all, 980 of the 1,406 (70%) CT scans were negative, while 426 (30%) were positive. Of these, 11 (3%) were followed up at one month, 354 (83%) were followed up at three months, 61 (14%) were scheduled for immediate workup with FNAC and CT.
Sixteen malignancies were diagnosed at 17 FNAC procedures. Of 56 total PET/CT scans, 33 were negative, 22 were positive, and one was indeterminate, resolved with FNAC.
"We had a diagnosis of malignancy in 23 cases … adenocarcinoma was the most frequent," Picozzi said. These included 10 (48%) non-small cell lung cancers (NSCLCs), eight (38%) stage 1A NSCLCs, three stage II NSCLCs, four stage III NSCLCs, two small cell lung cancers with limited disease, and one case of carcinoid disease.
In all, 19 of the 23 (83%) screening-detected cases were treatable.
The baseline screening results in the active arm of this study are similar to those of most observational studies, and the consistency of the results across continents and study criteria are cause for optimism that CT screening may be useful for identifying patients who can be treated, Picozzi concluded.
At present, "there is no evidence to recommend for or against screening, so the results of randomized trials are needed," she said.
By Eric Barnes
AuntMinnie.com staff writer
March 9, 2007
Related Reading
CT screening may not improve lung cancer survival, March 7, 2007
Overdiagnosis common in lung cancer screening, February 7, 2007
Endoscopic ultrasound tracks lung cancer, March 6, 2007
PET, CT CAD scheme differentiates benign from malignant lung nodules, November 28, 2006
CT lung cancer screening reduces mortality, October 26, 2006
Copyright © 2007 AuntMinnie.com