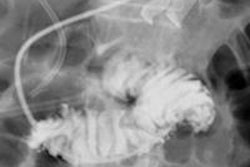
Digital x-ray firm Kubtec has launched its TomoView tomosynthesis technology for digital radiography of excised breast tissue.
The technology enables multiplanar imaging for margin analysis of excised breast tissue, and it is the core technology behind the company's upcoming Mozart product release, Kubtec said.
Mozart will provide imaging of excised breast tissue while increasing accuracy, saving time, and reducing re-excision rates in the operating room, the company said.
TomoView technology in Mozart allows one-step intraoperative margin analysis, eliminating the need for repositioning to obtain additional views, according to Kubtec. Mozart will therefore provide faster and more-efficient specimen radiology for surgery and pathology.
![Representative example of a 16-year-old male patient with underlying X-linked adrenoleukodystrophy. (A, B) Paired anteroposterior (AP) chest radiograph and dual-energy x-ray absorptiometry (DXA) report shows lumbar spine (L1 through L4) areal bone mineral density (BMD). The DXA report was reformatted for anonymization and improved readability. The patient had low BMD (Z score ≤ −2.0). (C) Model (chest radiography [CXR]–BMD) output shows the predicted raw BMD and Z score in comparison with the DXA reference standard, together with interpretability analyses using Shapley additive explanations (SHAP) and gradient-weighted class activation maps. The patient was classified as having low BMD, consistent with the reference standard. AM = age-matched, DEXA = dual-energy x-ray absorptiometry, RM2 = room 2, SNUH = Seoul National University Hospital, YA = young adult.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/04/ai-children-bone-density.0snnf2EJjr.jpg?auto=format%2Ccompress&fit=crop&h=100&q=70&w=100)




![Representative example of a 16-year-old male patient with underlying X-linked adrenoleukodystrophy. (A, B) Paired anteroposterior (AP) chest radiograph and dual-energy x-ray absorptiometry (DXA) report shows lumbar spine (L1 through L4) areal bone mineral density (BMD). The DXA report was reformatted for anonymization and improved readability. The patient had low BMD (Z score ≤ −2.0). (C) Model (chest radiography [CXR]–BMD) output shows the predicted raw BMD and Z score in comparison with the DXA reference standard, together with interpretability analyses using Shapley additive explanations (SHAP) and gradient-weighted class activation maps. The patient was classified as having low BMD, consistent with the reference standard. AM = age-matched, DEXA = dual-energy x-ray absorptiometry, RM2 = room 2, SNUH = Seoul National University Hospital, YA = young adult.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/04/ai-children-bone-density.0snnf2EJjr.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)









