General radiologists appear to be missing their chance to detect myocardial infarction (MI) during routine CT imaging. Researchers found that general radiologists prospectively detected fewer than half of MI on CT -- even though cardiac specialists found all of the cases when reviewing images after the fact.
Acute myocardial infarction occurs frequently -- in fact, it's the leading cause of sudden death in the U.S., with nearly 1 million cases uncovered in the U.S. each year, said Ashley Prosper from the University of Southern California's (USC) Keck School of Medicine in a presentation at the RSNA meeting earlier this month. Importantly, 21% of MI cases in the U.S. are clinically silent and therefore wouldn't necessarily trigger a patient encounter.
"Recently it has been suggested that by using conventional CT -- not even electrocardiogram-gated cardiac CT -- we can pick up signs of myocardial infarction," Prosper said. "Signs we can use to determine whether MI has taken place include low attenuation, calcifications, decreased enhancement, apical thrombi, and wall thinning."
Prosper said that USC researchers wanted to see how many myocardial infarctions could be found with conventional CT in a patient population in a large county institution. Prosper, along with Jabi Shriki, MD, and other colleagues from USC, examined patients who presented with chest pain or other symptoms, and who underwent conventional ungated cardiac CT as well as MRI over a two-year period. Cardiac MRI was used as the reference standard in the study.
All patients in the cohort had areas of late gadolinium enhancement at cardiac MR with morphology typical of MI. The conventional CT scans were obtained either before or after cardiac MR, and included any studies for clinical indications that included the heart, Prosper said.
Importantly, the conventional CT scans were initially read by general body radiologists, while experienced cardiac readers reviewed both the cardiac MR and CT studies (on separate occasions for each modality), according to Prosper.
The expert readers determined if areas of late enhancement were consistent with infarction. Infarcted areas (determined by low attenuation, myocardial calcification, decreased enhancement, wall thinning, and apical thrombi) were recorded separately for CT studies, and the studies were cross-checked to determine whether the same infarct areas had been identified.
In a total population of 252 patients who received cardiac MRI over the study period, 54 individuals also received conventional CT for comparison and were included in the study. A total of 27 patients who underwent both modalities were determined to have MI, including:
- 23 with areas of focal thinning and decreased perfusion
- 10 with areas of fat attenuation
- Three with thrombi
- Two with calcifications suggestive of infarction
Only 13 of 27 infarcts seen on conventional CT were identified by the original interpreting radiologists, Prosper said. The remaining infarcts were all identified by the experienced cardiac readers. Just six of 23 cases of focal thinning and decreased perfusion were identified in the original report, while three of 10 cases with lipomatous metaplasia were identified in the original report, and two of three with apical thrombi were seen at the initial reading, Prosper said. Both patients with myocardial calcifications were identified in the initial report.
"When we looked back to decide if certain characteristics of the infarcts had maybe pushed the original readers to state that there was an infarct, we didn't see any clear correlation between any specific characteristic and the reporting rate," Prosper said. Initial disagreement on the findings, resolved by consensus read, occurred in just two of 160 cases. In addition:
- Thirteen (48.1%) of the 27 infarcts seen on conventional CT were identified by the original interpreting radiologists.
- The remaining 14 infarcts were all identified retrospectively at CT by the experienced cardiac readers.
- Six (26%) of the 23 patients with focal wall thinning and decreased perfusion were recognized at the initial read.
- Three (30%) of 10 patients with lipomatous metaplasia were identified in the original reports.
- Two (66%) of three patients with apical thrombi were recognized in the initial read.
- Both patients with myocardial calcifications suggestive of MI were identified at the initial read.
The expert readers reported infarcts in different locations on two (0.62%) of the 160 cardiac MR studies (anterior versus septal in both). Study limitations included a long delay between CT and MR in some cases, Prosper said: a mean of 108 days for those who underwent CT before MRI, and a mean of 193 days for those who received CT after MRI. The small sample size and retrospective design were cited as additional limitations.
 |
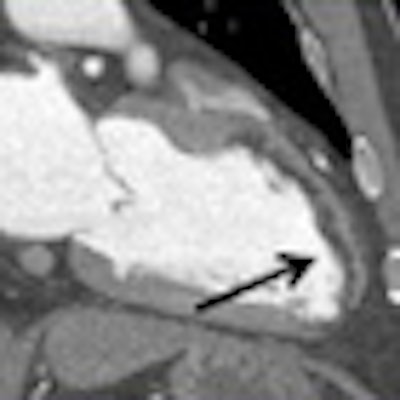
| In a 52-year-old man with right-upper-quadrant pain and leukocytosis, abdominal CT demonstrates gallstones (black arrow) and other findings suggestive of acute cholecystitis. Additionally, there is an area of anterior and apicoseptal wall thinning consistent with prior infarct. These regions also demonstrate delayed enhancement on postcontrast MR imaging. The cardiac findings were not discussed in the CT report. All images courtesy of Ashley Prosper and Jabi Shriki, MD. |
"We do not argue with the fact that cardiac MRI will remain the gold standard for detection of MIs; however, it's important to remember that the number of conventional CTs greatly outnumber them, and are much more widely accessible," Prosper said. "We suggest that radiologists maintain an appropriate index of suspicion when reviewing conventional CTs and take a look at the heart."
Particular attention should be paid to the attenuation and enhancement characteristics of the myocardium, and radiologists should be encouraged to report findings of myocardial infarction seen on conventional CT, she said.
Future study plans include an analysis of whether additional focused attention on the heart when reading conventional CT images can improve patient outcomes, Prosper said. A session moderator said it appears that body radiologists may need more training in the detection of cardiac findings.
Following her talk, Prosper, a fourth-year medical student, received an RSNA trainee research prize recognizing the study as an important contribution to research in radiology.
By Eric Barnes
AuntMinnie.com staff writer
December 29, 2010
Related Reading
Long after complicated pregnancy, maternal cardiac problems develop, December 22, 2010
Patients with suspected CAD and normal cardiac CT can 'sleep easy,' December 9, 2010
Simple calcium counting at chest CT predicts mortality risk, November 24, 2010
New cardiac CT guidelines expand use for low-risk patients, November 1, 2010
CT equivalent to IVUS for culprit plaque detection, December 4, 2008
Copyright © 2010 AuntMinnie.com