Barring evidence of cancer, patients who have undergone a failed colonoscopy can be successfully followed up with a reduced-prep virtual colonoscopy protocol. The study, by radiologists at the Stedelijk Ziekenhuis in Belgium, was presented at the 2004 European Congress of Radiology in Vienna.
"We know from previous studies that standard colonoscopic cleansing using polyethylene glycol (PEG) results in drowned patients, unhappy patients, and unhappy radiologists," Dr. Stefaan Gryspeerdt said. "Reduced colon cleansing with dietary fecal tagging results in happier patients, nicer images to look at, and happier radiologists."
Still, the researchers were less assured that failed colonoscopy patients, who may by definition have a greater incidence of colonic pathology or at least morphologic anomalies than those who undergo successful colonoscopy, could successfully undergo reduced-prep follow-up VC when same-day virtual colonoscopy was not practical.
Gryspeerdt, along with Dr. Philippe Lefere and colleagues, performed a study of virtual colonoscopy in 49 patients in whom conventional colonoscopy had failed to reach the cecum. Twenty-four of the 49 patients underwent a conventional cleansing regimen using a polyethylene glycol solution (59 g/l). The remaining 25 patients followed a low-residue diet for breakfast, lunch, and dinner (NutraPrep, E-Z-M, Lake Success, NY), in addition to 250 ml of a dedicated 2.1% barium tagging agent at the same three meals, cleansing with magnesium citrate and four bisacodyl tablets on the morning of the exam.
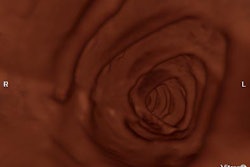
Following manual colonic insufflation with room air, all patients underwent prone and supine CT imaging on an eight-slice CT scanner (LightSpeed Ultra, GE Healthcare, Waukesha, WI) using 2.5 mm collimation and 1.3 mm reconstruction intervals. The images were evaluated on a workstation using endoluminal software.
"We looked for stool, fluid, and distension, looked whether or not residual material was tagged, and evaluated the results on the basis of Mann-Whitney U tests," Gryspeerdt said. "Stool, fluid, and distension were evaluated, and segmental stool was evaluated for prone and supine (imaging separately) as well as (for) a combined score," he said.
According to the results, "we found a trend toward more residual stool in the FT patients compared to standard cleansing (mean score 2.4 versus 2.5, respectively) which was not statistically significant," he said. "We didn’t find any difference in the size of the residual stool."
In terms of residual fluid, the FT group scored 3.8, compared to 7.2 for the standard cleansing group, a statistically significant difference (p<0.005). This was not surprising, however, since the magnesium citrate used in the FT group is a saline cathartic which has been shown to produce a drier prep than the polyethylene glycol lavage that was used in the standard-cleansing group.
Finally, the mean overall distension score was 0.12 for the FT group, compared with 2.5 for the standard-cleansing group, which was again statistically significant (p<0.005). Non-tagged stool was seen in only six segments in three patients, while non-tagged fluid was present in only four segments in three patients, Gryspeerdt said.
"However, one question remains: whether or not the observed differences in distension, residual stool, and residual fluids related to either the cleansing methods or the pathology," he said. "Therefore, we removed from calculations segments with diverticular disease, since diverticular disease causes incomplete distension. Moreover, tumoral disease should also be excluded, (as it) affects visibility and influences the distension of proximal segments."
When colonic segments were excluded for both the presence of pathology and poor distension, fecal tagging still resulted in more residual stool compared to standard cleansing, and the difference was statistically significant. As for residual fluid, the standard cleansing protocol still left more than the FT protocol, but the difference was no longer statistically significant, "probably due to the reduced numbers of patients and segments," he said. Finally, measurements of colonic distension no longer showed any difference between the standard cleansing and FT groups.
"(Virtual colonoscopy) with fecal tagging after incomplete colonoscopy is feasible," Gryspeerdt concluded. "With (colonic) redundancy, dolichocolon, or diverticular disease, the cecum...will probably never be reached." Virtual colonoscopy is therefore necessary for adequate assessment of the colon in such patients, he said, and as the reduced second prep is advantageous, it can be used effectively.
"However, in cases of malignancy, the setup of the entire abdomen with IV contrast is necessary because of staging the tumor, and we should avoid potential baroliths or barium impaction, which might be a reason not to use dietary fecal tagging which uses barium," he said. "And in case of malignancy it’s important to avoid a second preparation. So I think we should conclude that fecal tagging after incomplete colonoscopy is possible...but you should not use it in cases of tumoral disease."
By Eric BarnesAuntMinnie staff writer
April 7, 2004
Related Reading
New tagging, subtraction techniques aim for better compliance in VC, March 8, 2004
Experience sharpens role of IV contrast-enhanced VC, January 19, 2004
German group optimizes barium-sulfate tagging in MR colonography, January 22, 2003
Copyright © 2004 AuntMinnie.com