The triangular fibrocartilage complex (TFCC) is the main stabilizer of the distal radioulnar joint. As the carpi rotate over the radius and ulna, axial and shear forces are applied to the TFCC and injury, in the form of tears, can occur. The type of tear will influence imaging outcome.
Peripheral tears of the triangular fibrocartilage ulnar can be associated with instability of the distal radioulnar joint (DRUJ), which may go unseen on traditional MRI and/or arthroscopy. Two recent studies assessed the usefulness of MR arthrography in TFCC peripheral tears, offering some protocols and techniques for enhanced imaging.
In a related paper, a group from Switzerland and the U.S. looked at a possible association between carpal ligament injuries at MR arthrography and carpal instability at radiography.
Peripheral tears
First, Dr. Chen Shuang from Hua Shan Hospital and Shanghai Fudan University discussed his experience with direct MR arthrography for diagnosing TFCC tears at the 2006 RSNA meeting in Chicago.
For this study, 56 wrists were evaluated with direct MR arthrography and arthroscopy. Of these, 41 had peripheral TFCC tears. The remainder had normal radius or ulnar attachments that were confirmed by arthroscopy.
For direct MR arthrography, the needle was placed using clinical landmarks and fluoroscopy, Shuang said. Intra-articular injection was done at the radius-scaphoid space with 5-7 mL mixture of gadolinium and saline. In answer to RSNA session moderator Dr. William Palmer's question, Shuang said that image guidance was not routinely used at his institution for needle placement.
Three musculoskeletal radiologists assessed the MR images for TFCC tears at the radius or ulnar attachments, but were unaware of the arthroscopic results. According to the results, direct MR arthrography turned in a sensitivity of 87%, a specificity of 95%, and an accuracy of 91%.
 |
| The advantages of direct MR arthrography included clear visualization of synovial reaction and chondromalacia, and marrow edema, said Shuang and Xiaoyuan in their RSNA presentation. Images courtesy of Dr. Chen Shuang. |
 |
On MR arthrography, the readers saw high signal intensity of contrast media at the ulnar insertion or radius attachment of the TFCC. Synovial reaction, chondormalacia and marrow edema were also clearly depicted on T2-weighted imaging and direct MR arthrography.
Shuang and co-author Dr. Fen Xiaoyuan suggested that when assessing for peripheral TFCC tears, imagers would find more diagnostic value from the high signal intensity at the radius attachment than at the ulnar insertion. They concluded that direct MR arthrography can reveal the peripheral attachment of the TFCC. Shuang told AuntMinnie.com that direct MR arthrography is now the preferred modality for TFCC imaging at his institution.
In the second study, Dr. Christoph Rüegger and colleagues from Balgrist University Hospital in Switzerland, as well as the St. Louis-based Mallinckrodt Institute of Radiology, determined that contrast media must be injected directly in the DRUJ to achieve helpful MR results.
 |
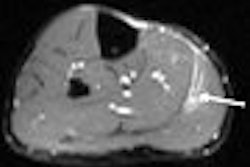
| A 19-year-old woman with noncommunicating tear of triangular fibrocartilage at ulnar insertion in right wrist due to fall off skateboard five months before examination. Arthroscopy showed communicating tear of triangular fibrocartilage at this location. Coronal T1-weighted image obtained with fat-saturated spin-echo sequence (TR/TE, 525/15) shows noncommunicating defect (arrow) in ulnar attachment of triangular fibrocartilage. |
For this study 41 patients with wrist pain underwent double-injection MR arthrography with two contrast agents (Iopamiro 3000, Bracco, Milan; Magnevist, Schering, Berlin).
"This approach of double injection into the DRUJ and the midcarpal joint is the routine MR arthrographic protocol at our institution," the authors explained. "Failure to inject contrast medium separately into the DRUJ can obscure the diagnosis of noncommunication ulnar-sided tear of the proximal surface of the triangular fibrocartilage" (American Journal of Roentgenology, January 2007, Vol. 188:1, pp. 187-192).
 |
| Same patient as above. Conventional arthrogram of distal radioulnar joint shows contrast agent pooling in triangular fibrocartilage defect (arrowheads). Rüegger C, Schmid MR, Pfirrmann CWA, Nagy L, Gilula LA, and Zanetti M. "Peripheral Tear of the Triangular Fibrocartilage: Depiction with MR Arthrography of the Distal Radioulnar Joint" (AJR 2007; 188:187-192). |
A 1.5-tesla MR system was used (Symphony, Siemens Medical Solutions, Erlangen, Germany) with the following sequences: coronal T1-weighted, fat-suppressed spin-echo; coronal proton density-weighted, fat-suppressed turbo spin-echo; sagittal T1-weighted spin-echo; and axial proton density-weighted turbo spin-echo.
The sensitivity for MR arthrography for finding ulnar attachment tears was 85%, specificity was 76%, and accuracy was 80%, according to the results. At MR arthrography, noncommunicating tears of the ulnar attachment were diagnosed in 19 patients and arthroscopy reveal peripheral tears in 14 of these cases. MR arthrography and arthroscopy spotted communicating tears in three patients. Finally, in 19 cases of normal attachment found on MR arthrography, arthroscopy noted three tears.
"The strength of MR arthrography with contrast injection into the DRUJ can be explained by the fact that this technique allows better differentiation of a tear from the physiologic high signal intensity caused by the vascularized ligamentum subcruentum," the authors explained.
Carpal instability
"The scapholunate ligament and lunotriquetral ligament are arguably the most important intrinsic carpal ligaments for maintaining carpal stability. Radiography provides only indirect information about ligament lesions.... With MR arthrography, the advantages of conventional arthrography and standard MR imaging are combined (with) greater accuracy (for) depicting intrinsic and extrinsic ligament injuries," wrote Dr. Nicolas Theumann from the Centre Hospitalier Universitaire Vaudois in Lausanne. Other co-authors are from the University of California, San Francisco, and the Mallinckrodt Institute of Radiology in St. Louis (Radiology, March 2006, Vol. 238:3, pp. 950-957).
For this retrospective research, data from 72 patients with post-traumatic wrist injuries were included. Of these, 28 underwent traditional arthroscopy after MR arthrography. Imaging consisted of the following:
- True neutral posteroanterior wrist radiographs
- Three-compartment arthrography with a 22-gauge needle, fluoroscopic guidance, and iodinated contrast agent (Magnevist, Schering)
- MR arthrography on a 1.5-tesla unit (Symphony, Siemens Medical Solutions) with a dedicated wrist coil
The MR protocol included sagittal T1-weighted spin-echo with fat saturation, transverse T1-weighted spin-echo with fat saturation, and 3D dual-echo steady-state imaging.
 |
| Above, posteroanterior radiograph of wrist in neutral position shows no evidence of scapholunate dissociation or carpal instability; alignment of both carpal rows is preserved. Below, conventional midcarpal arthrographic image of same wrist shows SLL (arrow) and central TFC (arrowhead) tears. |
 |
"High signal intensity visualized through the entire cross section of an extrinsic ligament was considered to indicate complete tear, whereas high signal intensity in only a part of the cross section of an extrinsic ligament was considered to indicate partial tear," the authors explained.
There were 25 triangular fibrocartilage (TFC) tears, 18 scapholunate ligament (SLL) tears, and 25 lunotriquetral ligament (LTL) tears, and 22 ligament tear lesions visualized in 60 patients at MR arthrography, according to the results.
 |
| Coronal 3D dual-echo steady-state MR image (60/10, 20˚ flip angle) findings in same wrist (as above) confirm presence of volar SLL (arrow) and central TFC (arrowhead) tears. "Association Between Extrinsic and Intrinsic Carpal Ligament Injuries at MR Arthrography and Carpal Instability at Radiography: Initial Observations," Theumann NH, et al. Radiology 2006;238:950-957. |
The authors noted that all intrinsic ligament tears seen at MR arthrography were confirmed in the 28 patients who also underwent arthroscopy. However, no extrinsic ligament tears were seen with arthroscopy. All extrinsic ligaments lesions were complete tears. There was a significant correlation between SLL tears LTL tears with carpal instability on x-ray, the authors added.
Nineteen patients had evidence of carpal instability on radiographs, while 27 had no sign of carpal instability, despite having at least one complete intrinsic lesion. Overall, 52% of these patients with at least one complete intrinsic lesion had no sign of carpal instability, leading the authors to conclude that "the carpal instability depicted on radiographs seemed to be related to the association between intrinsic and extrinsic ligament tears ... rather than to the presence of intrinsic ligament tears alone, even when the tears were complete."
In an e-mail to AuntMinnie.com, Theumann explained that MR arthrography can help steer patients toward the most appropriate treatment. MR arthrography "affects the treatment in the way that arthroscopy is (not) performed if nothing can be done, because the global status of the ligaments (intrinsic and extrinsic), cartilage, and bone bruise is better done with MRA than arthroscopy," he wrote. "If surgery is mandatory, the best and direct treatment is immediately available without any other procedure, like diagnostic arthroscopy."
By Shalmali Pal
AuntMinnie.com staff writer
January 19, 2006
Related Reading
MRI, US far from idle for hand, wrist injuries, November 6, 2006
Low-field dedicated extremity MRI useful for assessing early rheumatoid arthritis, September 8, 2006
Copyright © 2007 AuntMinnie.com