Patients with coronary artery plaques -- soft, mixed, or otherwise -- that go undetected in a calcium scan still have a good prognosis, according to a new study presented at last week's Society of Cardiovascular Computed Tomography (SCCT) meeting in Orlando, FL.
Researchers from St Luke's-Roosevelt Hospital in New York City took a closer look at more than 1,000 patients with zero calcium scores but with plaques found at coronary CT angiography (CCTA), hoping to determine if such patients might be falsely comforted by a zero calcium score if that had been their only test.
Gated calcium CT scans, which are acquired at low radiation dose levels and without contrast enhancement, are excellent at finding coronary artery calcium and determining the prognosis for adverse cardiac events. But calcium scans don't find all of the potentially dangerous plaques.
"We have always looked at calcium scoring as a test to rule out presence of atherosclerosis," said lead researcher Dr. Seth Uretsky, director of cardiac MRI and CT at St. Luke's-Roosevelt, in an interview with AuntMinnie.com. "We have found that by adding coronary CT angiography, there are, in fact, patients who have a zero calcium score but still have plaque detectable by CCTA."
The question, Uretsky said, is what the presence of undetected plaque means to patients with a zero calcium score. Are they at greater risk of cardiac events than patients without undetectable plaque?
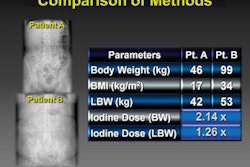
Researchers from St. Luke's-Roosevelt aimed to find out, using patient data from Advanced Cardiovascular Imaging, also in New York City. Uretsky, along with Advanced Cardiovascular's Dr. M. Robert Peters and colleagues, scanned patients referred for cardiac CT with a coronary artery calcium protocol, followed immediately by contrast-enhanced coronary CTA on a 64-detector-row LightSpeed VCT scanner (GE Healthcare, Chalfont St. Giles, U.K.).
Before the scans, patients practiced their breath-holds and received IV beta-blockade for heart rates greater than 65 bpm. CCTA was acquired using a low-dose step-and-shoot CCTA protocol yielding about 2-3 mSv for both scans.
"We've become very aggressive with radiation lowering," Uretsky said.
The study retrospectively evaluated 1,119 patients (51 ± 12 years, 52% male) without known coronary artery disease and a coronary artery calcium (CAC) score of zero. The researchers assessed age, gender, coronary artery disease risk factors, and the presence, morphology, location, and severity of coronary plaques at CT calcium scanning.
"What we found was that about 13% [n = 147) of our patients with a zero calcium score had plaque detected by coronary CTA," Uretsky said. "That's plaque of any kind. Most was noncalcified [n = 154, 73%] as you would imagine it to be [when] not detected by the calcium scan; however, there was a certain percentage of patients that did have calcified [n = 28, 13%] or mixed-morphology [n = 30, 14%] plaques."
The vast majority of CCTA-detected plaques were mild, including 184 (87%) plaques with stenosis less than 50%, 23 (11%) with stenoses of 50% to 70%, and only five (2%) with luminal diameter stenosis greater than 70% (i.e., approximately 50% cross-sectional narrowing).
"Only 2% of the overall plaques were severe, and only 0.4% of patients had severe plaques," Uretsky said. "Does the fact that you had plaques at CCTA that were not detected at coronary calcium portend a bad prognosis?"
Apparently not. Following the patients for two years after the scans, "only four patients out of the 1,119 died," Uretsky said. "The four patients who died were all in the group that had no plaque on coronary CTA. Not one patient with a zero calcium score with plaque on CCTA died," he said.
The researchers also performed receiver operator characteristics (ROC) analysis to assess the role of clinical factors in these patients. But beyond age and gender, analysis of coronary artery disease risk factors did not predict the presence of plaque.
Two years isn't a long follow-up period, but it's a good start, Uretsky said, adding that more research is needed to confirm that patients with undetected plaques at calcium scanning continue to enjoy low rates of adverse events.
The presence of luminal stenosis greater than 70% is rare in patients with plaques that are undetected by CAC scoring, he concluded. Moreover, the presence of coronary artery disease risk factors does not help to predict plaque presence among those patients with zero CAC scores.
"Although this was a retrospective study -- we only followed patients for two years -- I think it lends credence to the fact that in patients with zero calcium scores, you might miss plaque, [but] you could feel comfortable that these patients still have a good prognosis based on our study," Uretsky said.
Would it make sense to skip the calcium scan, spare these patients a little radiation, and go straight to low-dose coronary CTA?
"Right now the strongest prognostic data is based on calcium scoring," Uretsky said. "Coronary CT is still in infancy in that you don't have great prognostic data. [CCTA] gives you great information on what kind of plaque and what the stenosis is, but I still believe the calcium score is extremely useful in prognosticating patients."
By Eric Barnes
AuntMinnie.com staff writer
July 23, 2009
Related Reading
Prospectively gated coronary CTA nearly equals normal-dose scans, July 17, 2009
Repeated calcium scans increase cancer risk, study finds, July 13, 2009
Obstructive coronary artery lesions possible without calcification, July 1, 2009
CTA predicts coronary plaque instability, June 30, 2009
Absence of coronary calcium predicts excellent 10-year survival: study, June 18, 2009
Copyright © 2009 AuntMinnie.com