CT urography and cytoscopy are becoming the imaging team of choice for evaluating the urinary system, potentially replacing radiographic procedures such as intravenous or retrograde pyelography as often as 80% of the time, researchers report.
Urologists from Memorial Sloan-Kettering Cancer Center in New York City reported excellent sensitivity, but low specificity, in CT surveillance following radical cystectomy in 48 patients in a presentation at the 2004 American Urological Society meeting in San Francisco.
For a group from Innsbruck, Austria, thin-section MDCT yielded 97% accuracy in detecting diseases of the urinary tract. At the Cleveland Clinic Foundation in Ohio, doctors used multidetector-row CT to find the cause of macroscopic hematuria in 41% of the patients, but the group said that follow-up cytoscopy is still essential for finding the lesions CT misses.
"We were looking for a highly sensitive test to detect recurrences after cystectomy," Dr. Theresa Koppie told AuntMinnie.com. "Bladder cancer is a pan-urothelial disease, which means all the urothelium lining the kidneys, ureters, and bladder are at risk, as well as the urethra. So we tried to use this test to evaluate our patients and follow up if (cancer) could recur in these areas." Koppie is a urologist and research fellow at Memorial Sloan-Kettering.
All 47 patients in the study (mean age, 66.8 years) had undergone radical cystectomy with pelvic lymph node dissection following a diagnosis of bladder cancer; surgical diversions included an ileal conduit in 14 patients, orthotopic neobladder in 31 patients, and continent cutaneous diversion in two patients. The techniques for reconstructing the urinary tract are continually being refined, she said.
"Here the ureter would normally drain into the bladder, but instead the bladder is gone, and it diverts through something else," Koppie explained. "In this case we used a loop of bowel, which...comes out to the skin on their belly, or you can make a new bladder and connect it down to the natural anatomy connected to the penis, or in women to the perineum...It's a constant challenge, it's not perfect, but we've made a lot of changes in the surgery that have made it better."
For the study, all of the patients underwent postsurgical follow-up CT surveillance using either a LightSpeed or LightSpeed Ultra CT scanner (GE Healthcare, Waukesha, WI) at 5-mm collimation, and following the peripheral IV administration of 140 cc of iodinated contrast, Koppie said. Unenhanced, parenchymal, and excretory-phase images were acquired. Follow-up imaging occurred from six months to three years post-surgery. The mean delay was 26.8 months with a median of 11 months, and patients are now followed up yearly, Koppie said.
Follow-up CT after cystectomy is especially important in the presence of a positive urinary cytology, both for identifying upper-tract recurrence and for managing treatment, Koppie said; local recurrence is expected in about 5% of all patients.
The researchers evaluated the CT images for hydronephrosis, filling defects, strictures, thickening, renal pelvis, ureters, anastomosis, and periureteral soft-tissue changes. They found 13 cases of hydronephrosis, nine patients with filling defects ranging from 5 mm to 1.5 cm, and seven patients with periureteral stranding. Periureteral stranding occurred most commonly in the distal left ureter in the region where it crossed the left mesentery, she said. Calculi were found in two patients. Eight of the 47 patients had cancer recurrence, all histologically proven transitional-cell carcinomas obtained during open surgery, Koppie said.
"All of the patients who developed some kind of a cancer in the upper tracts (renal pelvis, calyces, ureter) had a positive CT urogram," Koppie said. CT was 100% sensitive, and 30.8% specific, for upper-tract disease recurrence.
"What that means is that there were a lot of false-positives; we would find a lot of things that didn't necessarily end up being cancer," Koppie said. "And that's important in some ways because in our patient population we really want to catch the lesions. So for us having a highly sensitive and low-specificity test is OK."
The CT protocol is becoming the standard follow-up for patients. A follow-up study will evaluate CT's performance in the absence of a positive cystology, Koppie said.
 |
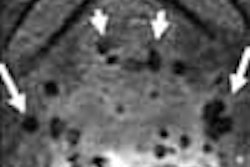
| Parenchymal phase (above), excretory phase (below), and MIP images (bottom) from a patient with a high-grade superficial recurrence of transitional cell carcinoma in the left renal pelvis. Images courtesy of Dr. Theresa Koppie. |
 |
 |
High sensitivity with thin-slice MDCT
In a study by Dr. Ammar Malouhi, Dr. Ferdinand Frauscher and colleagues from the University of Innsbruck in Austria, thin-section CT urography was 97% sensitive for the detection of urinary-tract disease in 45 patients.
The patients underwent CT imaging on a Sensation 16 scanner (Siemens Medical Solutions, Malvern, PA) using 16 x 1.25-mm slice thickness; multiplanar reconstructions were used for image review in all cases.
The 45 patients presented with two renal neoplasms, two parapelvic cysts, six ureteral calculi, two ureteral stenoses, two ureteral neoplasms, one case of double kidneys and one patient with a ureteral malformation. Of these, 34/45 patients with renal and kidney disease underwent the MDCT protocol. MDCT detected all upper-tract and bladder diseases in findings were confirmed by intravenous urography, retrograde pyelography, cystoscopy or ureterorenoscopy, except for a 3-mm bladder lesion that was missed.
In a general discussion of CT urography at the meeting, Franscher predicted that the modality should definitely replace IVP, but cautioned that thin-section imaging and multiplanar reconstructions are absolutely necessary to maintain high sensitivity.
"Five-millimeter (slices) are too big," he said. And if they are to pick up every last 3-mm lesion, the group will probably need to begin using 0.6-mm overlapping reconstructions, combined with low-dose protocols, he added.
Evaluating hematuria
In another AUA poster, researchers from the Cleveland Clinic Foundation in Ohio evaluated the use of CT for primary investigation of macroscopic hematuria (at least two specimens of three red blood cells per high power field (RCB/HPF) or greater), as a replacement for intravenous excretory urography.
The study, led by Dr. Justin Albani and colleagues, examined 31 patients (14 men, 17 women, ages 22-90, mean age 59) who underwent contrast-enhanced CT imaging using 3-mm collimation on a Siemens Somatom Sensation 16 scanner.
"It's a four-phase study" explained Dr. Nevidita Dhar, a resident and study participant from the facility. "Unenhanced, to rule out calcifications, then the arterial phase or nephrographic phase to see the collecting system, and then you get the late excretory phase, to help with hydronephrosis. It's kind of a functional study."
According to the results, 41% of the patients had an identifiable source of hematuria on CTU. Findings included one superficial papillary bladder tumor, three markedly enlarged prostates, on Bosniak II cyst, four renal calculi, and one papillary calyceal tumor. However, cystoscopy detected four cancers not seen by CTU, according to Dhar.
CT "doesn't replace cystoscopy, but (depicts) the collecting system anatomy as well as the parenchyma," in addition to incidental findings, she said.
"Our small study and others suggest that CT urography may offer a competitive alternative to intravenous excretory urography with its ability to opacify the collecting system and characterize renal parenchymal lesions in a singular exam," the authors wrote in an accompanying abstract. "It does not, however, replace the need for adjunctive cystoscopy to accurately identify bladder mucosal lesions that often are not detected on radiological evaluations."
By Eric BarnesAuntMinnie.com staff writer
June 18, 2004
Related Reading
Multidetector CT: Principles, Techniques, & Clinical Applications, April 13, 2004
Principles of Genitourinary Radiology, March 11, 2004
Multiphasic MDCT with contrast boosts liver, urography results March 1, 2004
Copyright © 2004 AuntMinnie.com