In a study that included all but the heaviest cardiac imaging patients, European and Japanese researchers were able to cut radiation dose by 31% in coronary CT angiography (CTA) studies by reducing the kilovoltage from 120 kV to 100 kV, with no difference in image quality.
What's more, the reduced-kV scans appeared to be equally effective at answering the clinical question at hand, without the need for additional tests from other imaging modalities.
"The rate of additional diagnostic tests like stress echo or myocardial perfusion imaging did not really differ," regardless of whether scans were acquired at 100 kV or 120 kV, said principal investigator Dr. Jörg Hausleiter from Deutsches Herzzentrum in Munich, Germany.
Hausleiter, a radiologist and professor of medicine at the center, discussed the Protection II (Prospective Randomized Trial on Radiation Dose Estimates of CT Angiography in Patients Scanned With a 100-kV Protocol) study at last month's Society of Cardiovascular Computed Tomography (SCCT) meeting in Orlando, FL, and by telephone with AuntMinnie.com.
The international, multicenter, and multivendor study aimed to evaluate the impact of 100-kV tube voltage on image quality and radiation exposure. A reduced tube voltage of 100 kV for coronary CTA has been shown to effectively reduce radiation exposure. The question was whether the image quality remained sufficient.
The study included patients who were scheduled to undergo coronary CTA with suspected coronary artery disease. Other major inclusion criteria were body weight less than 90 kg or body mass index (BMI) less than 30.
The study's primary end point was to demonstrate the equivalence in diagnostic image quality of the 100-kV protocol compared to 120 kV, while reducing radiation dose. A secondary aim was to show that additional tests would not be needed for the lower-dose 100-kV protocol, Hausleiter said.
A total of 400 patients with body weight less than 90 kg or BMI less than 30 and stable sinus rhythm were randomized to CTA with a tube voltage of 120 kV or 100 kV, Hausleiter said.
Seven imaging centers in Germany, Italy, and Spain used 64-detector scanners from GE Healthcare of Chalfont St. Giles, U.K.; Toshiba Medical Systems of Otawara, Japan; and Siemens Healthcare of Erlangen, Germany. The study did not use scanners from Philips Healthcare (Andover, MA), which released its 100-kV CTA protocol after the study began, Hausleiter said.
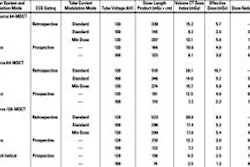
Automated exposure control, which had little effect on radiation dose in the Protection I study, was used at the discretion of the radiologist on site, Hausleiter said. Only the kV varied. About 90% of the studies were retrospectively triggered, while 10% used prospective gating. Beta-blockers were used at the discretion of the radiologist, and the mean heart rate of all patients was 56 beats per minute.
The investigators assessed diagnostic image quality on a four-point scale, ranging from 1, meaning nondiagnostic, to 4, meaning excellent image quality. Radiation dose estimates were derived from the dose-length product and a conversion coefficient for the chest (k = 0.014), Hausleiter said.
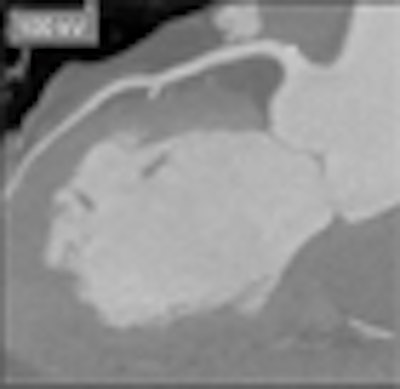
"In terms of image quality, the score was very much the same between the two groups," Hausleiter said. Image quality scores for the 120-kV scans were a mean of 3.30 (± 0.6), versus a score of 3.28 (± 0.68) for the 100-kV studies.
 |
| Curved-planar maximum intensity projections of the left descending artery demonstrate the image quality of the 100-kV (left) and 120-kV protocol (right) at identical window levels. Images illustrate the higher attenuation in the 100-kV scan protocol. All images courtesy of Dr. Jörg Hausleiter. |
The need for additional clinical tests, the secondary end point, did not differ significantly between the groups, he said. At the 30-day follow-up, the need for additional diagnostic tests was 19.2% with 120-kV acquisitions, versus 13.4% with 100-kV scans (p = 0.114).
Using the lower kV setting, mean radiation dose was reduced from 12.1 mSv with 120 kVp to 8.4 mSv with 100 kVp (p < 0.0001).
For the retrospectively gated exams, there is no reason the lower kV setting would not yield equivalent quality for assessing left ventricle or valve function, as well, according to Hausleiter.
"If you can image coronary arteries with high image quality, which is the most difficult thing, then you can also look at function," Hausleiter said. "But the question is coronary artery disease in these patients. We weren't looking at left ventricular function, which is easily obtained with echo."
As for study limitations, "it would be nice to see the diagnostic accuracy of both protocols to compare with invasive angiography," he said. "But if you wanted a meaningful number for diagnostic accuracy, we would have needed to enroll more than 1,600 patients ... which is completely undoable."
The coronary CTA protocol using 100 kV maintained high image quality while reducing radiation exposure by 31% compared to the standard 120-kVp protocol, Hausleiter concluded. The 100-kVp scans should be considered in all nonobese patients to keep radiation exposure as low as reasonably achievable.
A follow-up study, Protection III, that compares image quality in prospectively versus retrospectively triggered CTA exams has just been completed, and data are being analyzed, Hausleiter said.
By Eric Barnes
AuntMinnie.com staff writer
August 5, 2009
Related Reading
Peak voltage cut improves pulmonary CT angiography, July 22, 2009
Prospectively gated coronary CTA nearly equals normal-dose scans, July 17, 2009
High-pitch cardiothoracic CTA skips breath-holds and high doses, July 7, 2009
Repeated calcium scans increase cancer risk, study finds, June 13, 2009
Tube current modulation cuts triple rule-out CTA dose, April 15, 2009
Copyright © 2009 AuntMinnie.com