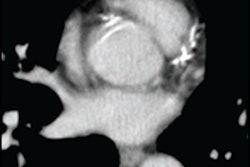
CT coronary artery calcium (CAC) testing is a useful and cost-effective way to develop a statin therapy strategy for African American patients who are at intermediate risk of atherosclerotic cardiovascular disease, according to a study published May 13 in JAMA Cardiology.
The findings offer an alternative to a blanket approach of initiating statin therapy in every person at risk, wrote a team led by Dr. Aferdita Spahillari of Massachusetts General Hospital.
"Coronary artery calcium testing may play a role in shared decision-making regarding statin use," the group wrote.
African Americans have greater incidence of atherosclerotic cardiovascular disease compared with their white counterparts, the authors noted. CT identifies the presence of CAC and helps clinicians classify disease risk in patients, helping them determine a statin therapy protocol.
But is using CAC assessment to determine preventive treatment for atherosclerotic cardiovascular disease cost-effective?
Spahillari's team addressed this question by comparing the 2013 American College of Cardiology/American Heart Association (ACC/AHA) guideline (which did not include a recommendation for CAC assessment) with the 2018 guideline (which recommended the use of CAC) for setting a statin treatment strategy in African American patients.
The group designed a model that included African American-specific data from 304 participants in the Jackson Heart Study at intermediate risk for atherosclerotic cardiovascular disease who underwent CAC assessment and received a score above 0; the authors used this model to calculate lifetime costs and quality-adjusted life years (QALYs) of CAC assessment.
Of the 304 patients, 178 (58.6%) had an assessment with a CAC score above 0. Using their model and the two scenarios (2013 versus 2018 recommendations), the group found the following:
- The 2013 guideline strategy translated to a greater QALY (0.0027) at a higher cost ($428.97) compared with the 2018 guideline strategy, with "an incremental cost-effectiveness ratio of $158,325 per QALY, which is considered to represent low-value care," the team wrote.
- The 2018 guideline strategy translated to greater QALY at a lower cost compared with the 2013 when patients preferred not to take daily medication. It was cost-effective in 76% of model simulations, with a value of $100,000 per QALY when there was a patient "preference to lose two weeks of perfect health to avoid one decade of daily therapy," the researchers wrote.
The study highlights the need for doctors to talk to their patients about disease prevention and management, wrote Eméfah Loccoh and Dr. Dhruv Kazi, both of the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology in Boston, in an accompanying editorial.
"For a patient who is willing to [take daily medication] ... universal statin therapy initiation may produce the best long-term health outcomes," the two wrote. "For a patient who is ambivalent about a daily preventive medication, a single CAC score may aid shared decision-making, with a CAC score of 0 suggesting that it may be acceptable to forgo the statin treatment."