X-ray imaging shows that corticosteroid injections for osteoarthritis pain in the hip and knee may actually damage the joints, leading to more rapid progression of the disease and eventually joint collapse, according to a study published online October 15 in Radiology.
The findings suggest that patients and their doctors need to be more aware of the risk of corticosteroid treatment for osteoarthritis, senior author Dr. Ali Guermazi, PhD, of Boston University School of Medicine, noted in a statement released by the RSNA.
"We've been telling patients that even if these injections don't relieve your pain, they're not going to hurt you," he stated. "But now we suspect that this is not necessarily the case."
Hip and knee osteoarthritis are common joint disorders and are often treated with injections of anti-inflammatory corticosteroids, which have long been considered safe, according to the researchers. But they found that these injections may actually accelerate the destruction of the joint, thus speeding up the need for hip and knee replacements.
Guermazi's team conducted a literature review to assess complications after treatment with corticosteroid injections, identifying four:
- Accelerated osteoarthritis progression
- Stress fractures beneath the cartilage
- Complications from death of bone tissue
- Rapid joint destruction, including bone loss
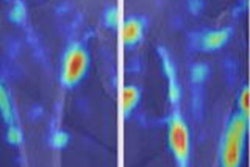
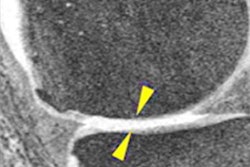
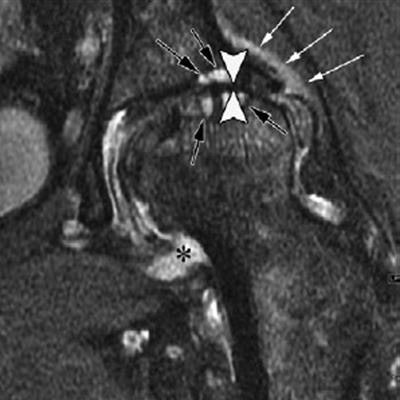
 Left: Anteroposterior left hip x-ray of a 61-year-old woman who presented with hip pain shows joint space narrowing (arrowheads) and femoral and acetabular osteophytic changes (arrows) consistent with hip osteoarthritis. Middle: Four months after intra-articular corticosteroid injection, anteroposterior hip radiograph shows severe interval joint space narrowing (arrowheads) and enlarging subchondral cysts (arrows). Right: Coronal intermediate-weighted fat-suppressed MRI obtained at the same time as middle image shows complete loss of the acetabular and femoral cartilage (arrowheads), with subchondral cystic changes (black arrows). In addition, there is joint effusion and synovitis (*) and periarticular soft-tissue edema (white arrows). This patient underwent total joint replacement three months later. Images courtesy of the RSNA.
Left: Anteroposterior left hip x-ray of a 61-year-old woman who presented with hip pain shows joint space narrowing (arrowheads) and femoral and acetabular osteophytic changes (arrows) consistent with hip osteoarthritis. Middle: Four months after intra-articular corticosteroid injection, anteroposterior hip radiograph shows severe interval joint space narrowing (arrowheads) and enlarging subchondral cysts (arrows). Right: Coronal intermediate-weighted fat-suppressed MRI obtained at the same time as middle image shows complete loss of the acetabular and femoral cartilage (arrowheads), with subchondral cystic changes (black arrows). In addition, there is joint effusion and synovitis (*) and periarticular soft-tissue edema (white arrows). This patient underwent total joint replacement three months later. Images courtesy of the RSNA.In light of these possible complications, the authors suggested that patients with mild or no osteoarthritis on x-ray who are referred for injections to treat joint pain be carefully tracked -- perhaps even with MRI.
"We believe that certain patient characteristics, including but not limited to acute change in pain not explained by using radiography and no or only mild osteoarthritis at radiography, should lead to careful reconsideration of a planned intra-articular corticosteroid injection," the group wrote. "In these circumstances, MRI may be helpful to further evaluate the actual cause of pain prior to a planned injection."
Since corticosteroids are so commonly used to treat joint pain, the repercussions of the study's findings could be huge -- and radiologists have a definite role in protecting the health of patients, according to the researchers.
"Given that intra-articular corticosteroid injections are increasingly performed to treat pain in patients with hip or knee osteoarthritis, we suggest that the radiologic community should actively engage in high-quality research on this topic to better understand potential at-risk conditions prior to intervention and to better understand potential adverse joint events after these procedures to avoid possible complications," the group wrote.
And even though patients may be willing to take the risk of joint damage from corticosteroid injections, they need to be informed, Dr. Richard Kijowski of the University of Wisconsin in Madison wrote in an accompanying commentary.
"Patients have the right to make this decision for themselves, and this requires radiologists to discuss all potential risks and benefits with the patient when obtaining written informed consent," he concluded.