Two groups of researchers have recently focused on improving gynecologic imaging as well as intervention. First, investigators from Turkey offer a case report on the multimodality diagnosis of endometrial stromal sarcoma in the myometrium. In the second paper, interventional radiologists discuss a potentially new way to perform nonsurgical fallopian tube occlusion.
Stromal sarcoma
In their case report, Dr. Ugur Toprak and co-authors tested out CT, MRI, and sonography for assessing low-grade endometrial stromal sarcoma. In addition, the 24-year-old patient had multiple nodular masses in the myometrium, as well as diffuse myometrial permeation.
"Endometrial curettage may not yield a significant result for low-grade endometrial stromal sarcoma because of its similarity to normal endometrial tissue," wrote the authors, who are from the Ankara Numune Education and Research Hospital in Ankara (American Journal Roentgenology, June 2004, Vol. 182:6, pp. 1531-1533).
The patient -- who had no previous genitourinary disease -- presented with abdominal fullness, menstrual irregularities, and an enlarged uterus. A transabdominal ultrasound revealed a left cornual, myometrial complex cystic mass with smooth borders.
 |
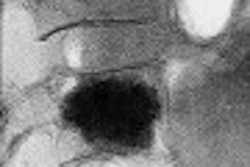
| Axial transabdominal pelvic sonogram shows complex myometrial mass with cystic and solid components. |
The CT exam with contrast showed heterogeneous enhancement of the solid components and septations of the corneal complex cystic lesions. T1- and T2-weighted MR scans showed isointense septations of the left cornual cystic lesions and small myometrial nodules. These same findings were hyperintense on gadolinium-enhanced MR.
Finally, "diffuse myometrial permeation of the right fallopian tube extended to the broad and round ligaments and invaded the peritoneum without any interruption," they said.
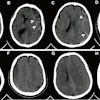
 |
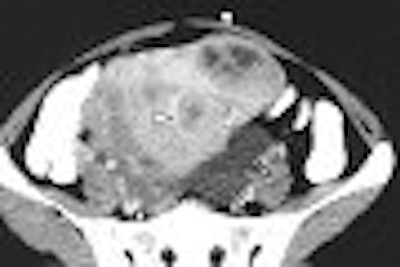
| Axial contrast-enhanced CT shows heterogeneous enhancement of solid components of myometrial nodules (solid arrowheads) and left adnexal peritoneal inclusion cyst (open arrowheads). |
The authors pointed out that each modality had its strengths and shortcomings in this particular disease. First, a definitive diagnosis was not possible with sonography because of nonspecific findings such as endomyometrial thickening.
In addition, uterine sarcoma has no specific features on CT to aid differential diagnosis. On MRI, it can be difficult to differentiate endometrial stromal sarcoma from leiomyosarcoma, which also has variable signal intensities on T2-weighted images.
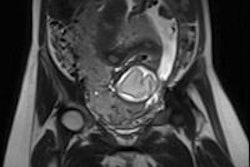
 |
| Axial T2-weighted MR image shows signal intensity of peritoneal inclusion cyst (solid arrowheads) appears to be brighter than that of ovarian cysts. Note left ovarian simple cyst and right ovarian follicle (open arrowheads). Toprak U, Pasaoglu E, Karademir MA, Gulbay M, "Sonographic, CT, and MRI Findings of Endometrial Stromal Sarcoma Located in the Myometrium and Associated with Peritoneal Inclusion Cyst," (AJR 2004 182; 1531-1533). |
The authors suggested keeping an eye out for the following imaging signs when dealing with a possible case of endometrial stromal sarcoma:
- Low-density mass with necrosis on CT
- Centrally hyperechoic cystic nodules on ultrasound
- Heterogeneous, prominent enhancement on contrast MRI because of rich vascularity
Fallopian tube occlusion
Inventing a less invasive way to perform sterilization continues to pose a challenge to women's health specialists. Currently, laparoscopic tubal ligation is performed with all the inherent risks of surgery, including inflammation, instability, and bowel or bladder injury.
Instead, the ideal occlusion device would avoid a severe reaction by firmly incorporating itself into the fallopian tube tissue, wrote Dr. Christoph Binkert and colleagues in the Journal of Vascular and Interventional Radiology. At the time of the study, the group was from Dotter Interventional Institute, Oregon Health & Science University in Portland. Binkert is now at Brigham and Women's Hospital and Harvard Medical School in Boston.
The investigators performed a pilot study of a porcine small intestine submucosa (SIS) device for fallopian tube occlusion. As this was an experimental study, rabbit models were used.
"SIS is an acelluar collagen-based material (with) the unique characteristic of inciting and supporting cellular ingrowth from adjacent tissues even as the SIS degrades," they explained (JVIR, June 2004, Vol. 15:6, pp. 609-613).
For this study, an SIS occluder was constructed of a loop-shaped frame of stainless steel wire, which was surrounded by a 5 x 2-mm piece of compressed SIS sponge, a radiopaque platinum wire, and an SIS layer.
"The initial challenge was to design an occluder that would stay in the fallopian tube," they said. "The occluder...was designed with two bare ends of a stainless-steel wire projecting beyond the SIS coverage. The barbs pointed against the peristalsis of the fallopian tube and were effective in preventing migration."
An initial hysterosalpingogram, with 5-7 mL of Oxilan 300 (Cook, Bloomington, IN), was performed to confirm tube patency in 16 adult female New Zealand white rabbits.
A 5-French coaxial micropuncture kit was used as the delivery system (Cook). The tip-mounted SIS occluder was advanced 1 cm into the fallopian tube, and the device was released. A saline solution was gently injected to moisten the device, causing it to expand, improving contact with the endothelium and anchoring the two wire ends. A follow-up hysterosalpingogram was then done immediately afterward, with a subsequent two-week x-ray follow-up.
According to the results, all occluders were successfully placed, with 15 remaining in the fallopian tube throughout the follow-up period. One device had migrated to the vagina. Histologic analysis showed complete filling of the fallopian tube with SIS material, and there was only one mild inflammatory reaction.
One pitfall of this technique is the fallopian tube's ability to recanalize around the SIS material, the authors said. A future improvement to the device might replace the steel wire with a copper wire to encourage complete fibrosis and complete tubal closure.
Continued animal testing of the device, using a copper wire, is planned, Binkert told AuntMinnie.com.
Other nonsurgical techniques that have been proposed include transcatheter RF electrocoagulation. A Korean team successfully performed transvaginal catheterization of the fallopian tube using a coaxial technique in 20 rabbits. They found that this method caused significant necrosis of the endosalpinx, as well as fibrosis of the occluded fallopian tube wall without tissue damage to adjacent organs (JVIR, April 2002, Vol. 134, pp. 399-404).
However, RF electrocoagulation would be limited to the central portion of the tube in order to protect surrounding tissue for radiation dose, Binkert said. The SIS device "would be safer, and could be applied more peripherally, which would make a re-anastomosis more likely to be successful."
By Shalmali PalAuntMinnie.com staff writer
July 2, 2004
Related Reading
Ultrasound supports conservative treatment of post-conception symptoms, April 27, 2004
PET proves versatile in imaging gynecologic cancer, August 4, 2003
Ultrasonographic diagnosis of tubal abnormalities, December 29, 2000
Copyright © 2004 AuntMinnie.com