When an infant or toddler is diagnosed with a bone fracture, is the injury the result of an accident, child abuse, or an old disease such as rickets making a comeback in modern society? Radiography can help radiologists make the distinction.
Pediatric radiologists and child abuse pediatricians at Seattle Children's Hospital report that bone fractures in mobile infants and toddlers diagnosed with rickets have telltale characteristics that differentiate them from nonaccidental trauma fractures caused by child abuse. But the researchers weren't able to find a correlation between cases of subclinical vitamin D deficiency and fractures -- a connection often made by defense attorneys in child abuse cases.
The researchers reported their results in a study published online in Pediatric Radiology (December 9, 2009).
Rising incidence
It's an unfortunate fact that cases of both rickets and child abuse are rising in the U.S., and radiologic interpretations may be the deciding factor when identifying the cause of bone fracture. In fact, radiologists have been asked to testify for both defense and plaintiff attorneys in abuse cases.
Much of the debate focuses on cases in which children have multiple fractures. Are such fractures a sign of abuse, or could they be caused by congenital conditions such as rickets, or even "brittle bones," as some defense attorney have claimed? And are there radiographic characteristics of rickets that might help radiologists distinguish between the condition and cases of child abuse?
The research originated at the request of pediatricians working in the Seattle Children's Hospital children's protection program, who asked the radiology department if a study could be conducted to identify the characteristics of bone fractures in children with rickets. They also wanted to determine if low vitamin D levels in infants could be the cause of fractures and to validate or disprove that "brittle bones" could generate such fractures.
 |
| Fracture in normal bone. Anteroposterior (left) and lateral (right) radiographs of the right femur in a 2-year-old with no metabolic bone disease demonstrates an acute displaced spiral fracture through the femoral diaphysis. Note the normal appearance of the metaphyses and growth plates, as well as normal bone mineralization. All images courtesy of Seattle Children's Hospital. |
Pediatric radiologists Dr. Teresa Chapman and Dr. Stephen Done began the project in the summer of 2008. In addition to addressing the requests from their colleagues, they expanded the objectives to include identifying the age at which bone fractures occur in children diagnosed with rickets, and to determine the percentage of children with rickets who developed rickets-related fractures.
The research team reviewed the medical records of children younger than 24 months diagnosed with rickets, who had been treated for any reason at Seattle Children's Hospital from January 2000 through June 2008. They used a database search of both laboratory test reports and radiology reports to identify the children, whose medical records and x-rays were then thoroughly reviewed.
Forty-five children were identified as having rickets, with 80% having a diagnosis of nutritional rickets. More than half of the children with nutritional rickets were African-American or the children of African immigrants. Half of the children with congenital or secondary rickets were Caucasian.
The children ranged in age from 2 to 24 months, with a mean age of 13 months. Five children were excluded from the study, because they either had no radiographic evidence of rickets or unknown causes of rickets.
Of the remaining 40 children with nutritional, congenital, or secondary rickets, seven (17.5%) had bone fractures. Two children had one fracture; the remainder had up to three fractures. The children were 8 to 19 months of age and were independently mobile. Six of these children had abnormally low vitamin D levels, and all seven had obvious rickets-related changes with widespread metaphyseal fraying and cupping.
The fracture types in the seven children with rickets were characterized as being transverse diaphyseal, metaphyseal, and lateral or anterior-lateral rib fractures, all resembling structural insufficiency fractures. Fractures were consistent with a failure of load-bearing and occurred in areas of abnormal bone, the authors reported. None of the children had vertebral fractures, classic metaphyseal lesions, or skull fractures.
 |
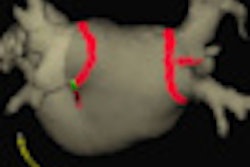
| Fracture in rachitic bone. Anteroposterior radiograph of the bilateral knees in a patient with severe rickets demonstrates diffuse osteopenia and subtle cortical irregularity at the distal left femur, consistent with a nondisplaced transverse fracture. |
Unanswered questions
While the study helped the researchers gain insight into rickets-related fractures, they were ultimately unable to address the issue of whether "brittle bones" caused by vitamin D deficiency could lead to cases of multiple fractures. Complicating the issue is the fact that some children with severe vitamin D deficiency never develop rickets at all.
Indeed, the patient cohort in the study was small, and there were no infants younger than 6 months who developed fractures, the researchers said.
"We treat many children with vitamin D deficiency and insufficiency at Seattle Children's Hospital, but only a small portion of these children develop rickets, and a smaller proportion of children with rickets develop fractures," Chapman said. "Our study shows that severe rickets predisposes to fractures in mobile infants and toddlers, but we were unable to correlate fractures with vitamin D levels."
That said, radiologists should still be able to tell the difference between rickets-related fractures and cases of child abuse.
"We are confident that radiologists familiar with the infant skeleton would not have difficulty recognizing the underlying metabolic bone disease," the authors wrote.
The researchers encourage radiologists at other pediatric hospitals to conduct similar studies to further investigate this subject.
By Cynthia E. Keen
AuntMinnie.com staff writer
January 18, 2010
Related Reading
Occult abdominal trauma common in children with suspected physical abuse, November 25, 2009
Chest x-ray measures up to CT for pediatric blunt chest trauma, July 17, 2009
Copyright © 2010 AuntMinnie.com