Article Summary
Researchers identified a CT imaging sign called the hyperdense capsule sign that helps predict which subdural hematoma patients will benefit most from a minimally invasive procedure called middle meningeal artery embolization, reducing recurrence rates from 12% to 5% in eligible patients.
- The hyperdense capsule sign is a linear, hyperdense layer visible on standard CT scans along the inner membrane of subdural hematomas
- Among 697 study participants, 63.7% showed the sign, and those with it experienced significantly lower recurrence rates after embolization (5.0% vs 12.0%)
- Patients with the sign also experienced fewer serious adverse events after treatment (5.9% vs 15.1%) compared to standard care
- The sign provides a cost-effective, non-invasive screening tool requiring only a standard noncontrast CT scan to identify ideal candidates for the procedure
- Further prospective studies are needed to validate these findings and explore long-term effects in this patient population
Researchers have identified a sign visible on CT scans that may help identify which patients are likely to benefit from embolization for subdural hematomas, according to a study published in the July 7 issue of Radiology.
In a post-hoc analysis of randomized trial involving 697 participants, those with the sign -- named “the hyperdense capsule sign” -- had less than half the rate of hematoma recurrence or progression after middle meningeal artery embolization (MMAE) than those without it, noted lead author Ruiyuan Weng, MD, of Fudan University in Shanghai, and colleagues.
“Overall, the [the hyperdense capsule sign] provides surgeons a convenient and cost-effective radiologic risk stratification tool to help identify potential candidates for MMAE, as a simple noncontrast CT scan can be performed to determine its presence or absence,” the group wrote.
Nonacute subdural hematomas recur or progress in 5% to 37% of cases after standard treatment, and recent trials of MMAE have shown mixed results, which the authors noted may reflect unrecognized differences among patients. The hyperdense capsule sign (HDCS) is a linear, relatively hyperdense layer visible along the inner membrane of a subdural hematoma, and in this analysis the researchers hypothesized that it could be used to screen for patients who may benefit from MMAE.
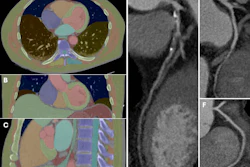
 Representative axial noncontrast CT images with and without the hyperdense capsule sign (HDCS). The HDCS is defined as a hyperdense capsule layer of linear shape surrounding a subdural hematoma (SDH). (A–D) Images of SDH with the HDCS (arrowheads). (E–H) Images of SDH without the HDCS.RSNA
Representative axial noncontrast CT images with and without the hyperdense capsule sign (HDCS). The HDCS is defined as a hyperdense capsule layer of linear shape surrounding a subdural hematoma (SDH). (A–D) Images of SDH with the HDCS (arrowheads). (E–H) Images of SDH without the HDCS.RSNA
In addition, the proportion of participants experiencing a serious adverse event was lower in the embolization versus usual-care group among those with the HDCS (5.9% vs 15.1%, p = 0.002) but not among those without the HDCS (8.7% vs 5.6%, p = 0.34), the researchers reported.
“Among participants with the HDCS, adjunctive MMAE resulted in significant benefits over usual care, including a lower incidence of symptomatic recurrence or progression within 90 days and fewer serious adverse events,” the group wrote.
The HDCS is a radiologic feature that, to their knowledge, has not been previously reported, and cautious interpretation is warranted, the researchers noted.
“Further prospective randomized studies are warranted to validate these results and explore the long-term effects of MMAE in patients with the HDCS,” the group concluded.
In an accompanying editorial, David Kallmes, MD, of the Mayo Clinic in Rochester, MN, noted that the investigators have introduced an intriguing and potentially useful imaging biomarker.
“While further validation is required, their work contributes meaningfully to the ongoing effort to refine and personalize the management of chronic [subdural hematoma],” he wrote.
The next phase of investigation should focus not only on validating individual markers, but also on integrating imaging, clinical, and procedural variables into cohesive predictive frameworks capable of guiding real-world decision-making and optimizing patient outcomes, Kallmes concluded.
The full study is available here.