Neuroradiological manifestations of COVID-19 differ by the severity of the disease, according to a literature review published August 29 in Academic Radiology. The results could help clinicians better understand neurological expressions of COVID-19.
"An increasing number of neurological complications and corresponding radiological findings have been reported in patients with COVID-19 infection," wrote a team led by Simon Pan, PhD, of the University of California, San Francisco. "[We sought] to systematically review the current literature on COVID-19-associated neuroradiological findings and examine the prevalence of different findings in patients with both severe and mild COVID-19 infection."
Pan and colleagues conducted a literature search of PubMed and Embase, gathering 61 studies published between 2019 and 2020 that reported CT and MRI neuroimaging findings in 711 patients with confirmed COVID-19 disease. The group tracked patient demographics, main imaging findings, neurological symptoms, and severity of COVID-19 disease.
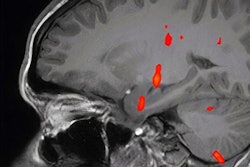
Common neurological findings in patients with mild illness included the following:
- Cranial nerve abnormalities
- Ischemic infarction
- White-matter abnormalities
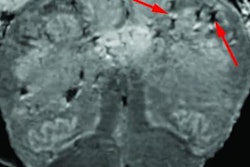
Common findings in patients with severe disease included the following:
- White-matter abnormalities
- Ischemic infarction
- Hemorrhagic events
"Cranial nerve abnormalities appear exclusive to mild infection, with a high degree of olfactory tract involvement, while hemorrhagic events are more common in severe infection," the team concluded. "Notably, ischemic infarction was equally prevalent in both mild and severe COVID-19 infection. Healthcare providers treating COVID-19 patients should be aware of these potential complications and consider neurological assessment and neuroimaging studies when indicated."