Vasculopathy in the form of diffuse intimal proliferation is the biggest cause of late death among heart transplant patients. The telltale intimal thickening can be seen on intravascular ultrasound, but rarely at angiography and quite readily at MDCT. The modality's sensitivity for detecting intimal thickening and significant stenosis make it an excellent choice for screening post-transplant patients, according to researchers from Argentina.
"Heart transplant patients commonly develop asymptomatic coronary disease, and these patients require frequent screening," said Dr. Patricia Carrascosa from Diagnóstico Maipu in Buenos Aires. "In general, they are evaluated by invasive angiography and by intravascular ultrasound."
But these modalities are invasive and associated with an increased rate of complications, creating the need for a noninvasive alternative, she said.
"It's important to evaluate the lumen as well as the diffuse endothelial (aka intimal) proliferation, which is not identified with only a venogram," Carrascosa said in a presentation at the 2005 RSNA meeting in Chicago.
In a study of transplant patients, the researchers sought to determine the role of multidetector-row CT (MDCT) in the coronary artery evaluation compared to intravascular ultrasound (IVUS) and invasive digital subtraction angiography (DSA).
Other studies have examined the role of risk co-factors, genetics, and suppressive agents on the development of coronary allograft vasculopathy.
CT versus IVUS, DSA
"We evaluated a group of 19 heart transplant patients, and we correlated the results with conventional angiography," Carrascosa said. "Fifteen of these patients also had intravascular ultrasound performed." CT segments considered true-negative by digital angiography (stenosis less than 50%) were compared with IVUS to establish intimal proliferation.
CT angiography images were acquired on a Brilliance 16 scanner (Philips Medical Systems, Andover, MA) at 16 x 0.75-mm collimation, 500 mAs, 140 kVp, 0.428-sec rotation, and 0.5-mm reconstruction interval, following administration of 100 mL of iodinated contrast by power injector. Automated exposure control beginning at 150 HU enabled good visualization of the coronary arteries, she said.
"After the acquisitions, we reconstructed four phases: two diastolic phases at 70% and 25%, and two systolic phases at 40% and 50%," Carrascosa said.
IVUS was performed with an Ultra Cross 3.2 F 30-mHz coronary imaging catheter (Boston Scientific, Natick, MA). All patients had previously received a bolus of 70 IU/kg of unfractioned heparin and 0.2 mg of nitroglycerin intra-arterially.
"We did not give any beta blockers to the patients, as it is known that transplant patients do not respond to beta blockers," she said. Nevertheless, variability in heart rate was very low.
Cross-sectional images from both methods were matched via distance (10 mm) from the ostium up to the vessel reaching a diameter of 1.5 mm, the group wrote in an accompanying abstract. Two readers working independently evaluated the results (though most MDCT studies were read by a single reader), and the exact binomial method was used to calculate sensitivity, specificity, and positive and negative predictive value for each modality.
"Only four segments were not evaluable by MDCT due to motion artifacts, and all were located in right coronary arteries," Carrascosa said.
Compared to angiography, MDCT yielded 20 true-positive segments, 294 true negatives, two false positives, and three false negatives, with a sensitivity of 87% (CI 65.3%, 96.6%), positive predictive value of 90.9% (CI 69.4%, 98.4%), and negative predictive value of99.0% (96.8%, 99.7%).
MDCT compared to intravascular ultrasound yielded 51 true-positive segments, 151 true negatives, 20 false positives, and five false negatives. Its sensitivity was 91.1% (CI 79.6%, 96.7%), specificity 88.3% (CI 82.3%, 92.5%), positive predictive value 71.8% (CI 59.7, 81.6), and negative predictive value 96.8% (CI 92.3, 98.8). There were no complications in any of the patients studied.
In images of a 62-year-old patient who underwent a heart transplant in 1999 due to cardiomyopathy, a heart rate of 115 bpm did not render the CT data nondiagnostic.
On CT "we observed on the axial images mixed plaque in the distal portion of the main LAD (left anterior descending), calcified soft plaque … at the LAD, and correlation between (CT and) IVUS where we observed the soft portion of the plaque," Carrascosa said. "On digital angiography we cannot determine any stenosis on distal portion of main LAD so this is a negative finding for conventional angiography in correlation with (MDCT)."
 |
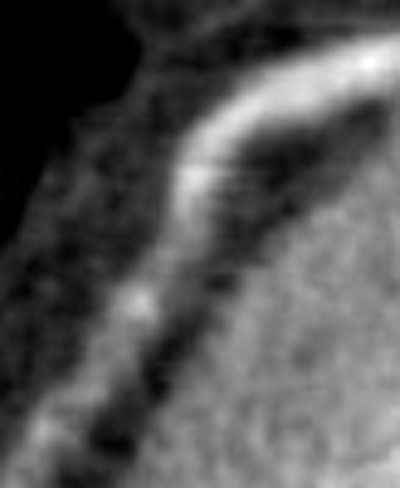
| Top to bottom: Endothelial proliferation in a transplant patient. Above, normal digital angiography . Below, MDCT multiplanar curved reformation of left main artery and left anterior descending artery; arrow points to area of endothelial proliferation. Next, IVUS followed by (bottom) axial CT image at the same level demonstrating endothelial proliferation. All images courtesy of Dr. Patricia Carrascosa. |
 |
 |
 |
In a second example, a 60-year-old patient who underwent a heart transplant in 2000 due to systemic cardiomyopathy had subtle endothelial proliferation in the artery that could be seen in the multiplanar reformatted image of the right cerebral artery, which was correlated to the IVUS images. The intimal proliferation "does not produce stenosis, but it's diffuse and we see the vessel with (a smaller) diameter," Carrascosa said.
"The evaluation of vasculopathy is done very well with MDCT because it's valuable for the difficult identification of luminal stenosis, and can rule out the presence of intimal proliferation from transplantations," she concluded. "It also allows a noninvasive evaluation of cardiomyopathy in these patients."
Vasculopathy not created equal
A study in the Journal of Heart and Lung Transplantation found that the presence of severe intimal thickening alone was not a good predictor of cardiac events, suggesting that co-factors such as hyperlipidemia may play an important role. Mehra et al studied heart transplant patients with severe intimal thickening for two years.
"Not all heart transplant recipients who exhibit a 'prognostically relevant' threshold of severe (greater than 0.5 mm) intimal thickening experience cardiac events," they wrote. "We sought to contrast clinical characteristics of heart transplant recipients who have prognostically relevant, severe intimal proliferation and who experience cardiac events with those who remain event-free" (Journal of Heart and Lung Transplantation, February 2003, Vol. 22:2, pp. 118-123).
They examined 54 heart transplant recipients with severe intimal proliferation (intimal thickness greater than 0.5 mm) of the coronary arteries at index IVUS examination to assess the development of cardiac events (sudden cardiac death, myocardial infarction) and the need for percutaneous coronary revascularization via angioplasty, atherectomy, stent implantation, or surgical bypass.
At two years there were 33 patients with no events and 22 with cardiac events. Both groups showed similar intimal thickness at IVUS (group 1, 0.89 ± 0.27 mm versus group 2, 0.94 ± 0.36 mm; p = not significant). However, the group with cardiac events were likelier to have hyperlipidemia, to have greater exposure to cumulative and average daily prednisone, and to exhibit greater average biopsy rejection scores at follow-up.
The results "underscore the importance of the quality and not merely the quantity of intimal proliferation in determining occurrence of morbid cardiac events," and "further emphasize the interaction of immunologic and nonimmunologic factors in determining event vulnerability in cardiac allograft vasculopathy," Mehra and colleagues wrote.
Preventing tissue proliferation
Animal studies have looked at agents that might potentially suppress chronic vascular rejection and thus intimal proliferation in transplant patients.
Balsam et al hypothesized that early inhibition of apoptosis with a caspase-3 inhibitor would also lessen the development of graft coronary artery disease. Donor hearts from rats were pretreated with 50 micrograms of DEVD-CHO, a cell-permeable caspase-3 inhibitor, or a vehicle. The recipient animals were pretreated with 1.7 mg/kg of intraperitoneal DEVD-CHO, an inhibitor, or a vehicle, along with cyclosporine to prevent acute rejection.
"At 90 days, intimal proliferation was significantly higher in vehicle-treated animals than in inhibitor-treated animals," they wrote. The percentage of vessels with high-grade occlusion (greater than 50%) was also lower in inhibitor-treated animals (Journal of Heart and Lung Transplantation, July 2005, Vol. 24:7, pp. 827-832).
Statins may also exert a protective effect. A Japanese study found that in seven rabbits, pravastatin significantly suppressed vein graft intimal hyperplasia in vivo via endothelial cell-tropic Rho-kinase inhibition. The results "strongly support the clinical use of hydrophilic statins to prevent intimal hyperplasia of the vein graft after bypass grafting," Yamaonuchi et al wrote (Journal of Vascular Surgery, October 2005, Vol. 42:4, pp 757-764).
By Eric Barnes
AuntMinnie.com staff writer
February 27, 2006
Related Reading
Colorectal complications may follow heart and lung transplantation, January 26, 2006
IVUS may spot potential "culprits" among coronary calcium deposits, January 4, 2005
MDCT evaluates vasculopathy in transplanted hearts, December 7, 2004
Copyright © 2006 AuntMinnie.com


















