Monitoring elderly and frail patients during bowel preparation appears to be a prudent way of avoiding problems with virtual colonoscopy (CT colonography [CTC]) exams, according to a new study from Ireland. While most patients 70 years and older took their cathartic prep in stride, a few with minor irregularities such as electrolyte imbalances convinced the investigators they were on the right track with monitoring.
"Unfortunately, we don't have definite guidance regarding the metabolic safety of full mechanical bowel prep in CTC of elderly and frail patients," said Patrick McLaughlin, of Cork University Hospital in Cork, Ireland, in a presentation at the 2007 RSNA meeting in Chicago. "The existing case reports and ... reports in the literature are largely confined to optical colonoscopy. (There is) a question of relevance to CTC, where bowel prep may be of a different duration, may be a different regimen, and also the administration of IV contrast material is an additional potential risk associated with CTC."
There is evidence that VC is worth doing in the elderly, and may even offer unique benefits, McLaughlin said, citing a 2007 study from the American Journal of Roentgenology.
In that study, Tolan and colleagues from St. James's University Hospital in Leeds, U.K., replaced barium enema with virtual colonoscopy in 400 patients 70 and older. VC revealed previously unknown extracolonic lesions in 96 of 400 patients (24%). Of these, 49 patients (12.3%) had a previously unknown malignancy, including 29 extracolonic and 23 colorectal cancers (AJR, November 2007, Vol. 189:5, pp. 1104-1111).
Complications are quite rare, but risks are associated with the full bowel prep, which is known to deliver higher sensitivity and specificity compared to reduced prep protocols, McLaughlin said.
 |
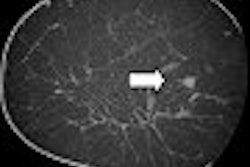
| Inadequate bowel preparation at VC is especially problematic in elderly patients. All images courtesy of Patrick McLaughlin. |
"In our experience, these can be especially problematic in elderly patients. However, in day-to-day practice, side effects associated with mechanical bowel prep and incomplete bowel preparation may not be as obvious," McLaughlin said. "They include dehydration, renal function disturbances, and electrolyte disturbances, of which there have been case reports of fatalities."
Two recent review articles (Greene J. et al, British Society of Gastroenterology, November 2006; Canadian Journal of Gastroenterology, November 2006, Vol. 20:11, pp, 699-710) reported that these risks are greatest in the elderly, those with cardiac failure, renal failure, and hypertension.
The take-home message from these reports: "Particular care is required to avoid excessive fluid and electrolyte shifts in these groups," McLaughlin said. "Our study aimed to retrospectively evaluate the metabolic safety of full-preparation CTC in a subgroup of frail and elderly patients."
Over a period of 36 months, 559 patients underwent virtual colonoscopy, 143 of whom (46%) were 70 years or older. From this group, the researchers selected 78 patients (mean age 78, range 70-91) with a high incidence of medical co-morbidity that included congestive heart failure, impairment, hypertension, and history of malignancy, McLaughlin said.
All patients went on a low-residue diet beginning five days before the procedure. Two days before scanning they underwent a bowel preparation consisting of 40 mg of sodium picosulphate magnesium citrate (Picolax, Ferring Pharmaceuticals, Langley, U.K.), given in four divided doses. All patients received IV administration of nonionic contrast (90-100 mL of 300 mg i/mL) and IV rehydration before scanning.
"We retrospectively reviewed all medical records and recorded vital parameters, including serum sodium potassium, urea (and creatinine), at three days prior and one-day postexamination," McLaughlin said. Statistical analysis was conducted using Microsoft Excel 2007 and SPSS version 15.
Prior to the bowel preparation, electrolyte findings were normal in the majority (n = 71, 91%) of patients, McLaughlin said. Seven patients (9%) had electrolyte disturbances that resolved in six patients and deteriorated in one patient. As for baseline renal function, 43 patients (55%) were normal and 35 patients (45%) were abnormal (average deterioration: 12 mmol of serum creatinine, 1.2 mmol of serum urea).
After the bowel prep began, two patients developed renal function disturbance with peak serum creatinine levels of 134 mmol (normal: 50-130 mmol) and peak serum urea levels of 7.5 mmol (normal: 2.5-7 mmol).
"There were 10 new cases (12.8%) of electrolyte disturbances within the bowel prep period, including four cases of hyponatremia, one case of hypernatremia, four cases of hyperkalemia, and one case of hypokalemia," McLaughlin said. Most were mild and clinically insignificant, but two cases of hyperkalemia required pharmacologic intervention. Still, no patients required dialysis during the procedure, McLaughlin said.
 |
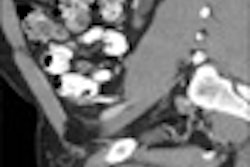
| Results showed that most changes in renal function and electrolyte balances were mild and self-resolving after the procedure. However, two cases required pharmacologic intervention. |
 |
The main limitations of the study were its retrospective design, the confounding factor of IV administration, and the lack of a control group, he said.
"In light of fact that we do not have definitive guidance for safety in full bowel prep in CTC, in current practice, we concluded that in frail and elderly patients, performing CTC (on) inpatients allows early detection of electrolyte disturbances during bowel preparation," McLaughlin said. In this cohort of patients, VC appears to result in safe practice and satisfactory patient outcomes, he said.
"We are continuing to collect data prospectively with the aim of identifying 'at risk' subgroups of elderly patients in whom full oral bowel preparation may be metabolically unsafe to prescribe," McLaughlin wrote AuntMinnie.com in an e-mail.
By Eric Barnes
AuntMinnie.com staff writer
January 28, 2008
Related Reading
Bowel prep with sodium phosphate or PEG pose low risks of renal impairment, January 4, 2008
Unusual VC regimen a success in the elderly, November 27, 2007
VC in elderly patients yields extracolonic advantage, November 7, 2007
Extracolonic findings double VC costs, but might be worth paying, July 20, 2006
Tagged VC succeeds where colonoscopy fails in elderly, March 28, 2006
Copyright © 2008 AuntMinnie.com