Does vertebroplasty reduce patients' pain? The literature shows unequivocally that it does. Yet there is ongoing debate about the cause and rate of new fractures found after the interventional procedure, and whether vertebroplasty alone can augment vertebral body height.
On the last question, however, researchers from Germany are confident the answer is yes.
Dr. Johannes Hierholzer, a professor of interventional radiology from the University of Potsdam, led a study that examined the ability of vertebroplasty to enhance vertebral body height.
After excluding malignant cases, the group performed vertebroplasty bilaterally on 102 vertebral bodies in 70 consecutive patients with symptomatic osteoporotic collapse. The group uses as little cement as possible, 2-3 cc per injection, Hierholzer said at the 2006 European Congress of Radiology (ECR) in Vienna.
Three-dimensional volume measurements were performed at nine points on preoperative MRI and again on postoperative CT, and the results were correlated with clinical features.
"We chose nine points -- at the posterior border, anterior border, and middle of the vertebral body," Hierholzer said. Following the normal clinical protocol at his facility, different imaging modalities were used before and after the procedure.
Postoperative follow-up included physical examination and acquisition of multidetector-row CT (MDCT) data (Sensation 16, Siemens Medical Solutions, Erlangen, Germany) using 0.75-mm slices, multiformat reconstruction of maximum intensity projection (MIP) images in sagittal, axial, and coronal planes.
"We had to compare MRI preop with CT reformatted images postop ... with the three MRIs: medial, left, and right sagittal plane, and the corresponding CT slices plus (assessment of) the kyphotic angle," Hierholzer said. The measurement method was validated with the comparison of control imaging data from the same nine data points in untreated vertebral bodies.
"As we expected, we did not have a significant change in height in the untreated bodies, and there was no significant increase in absolute or relative measurements ... so we think the methodology can be regarded as robust," he said.
 |
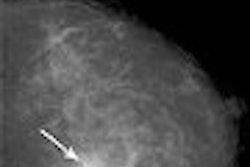
| Preoperative MRI (above) and postoperative CT (below) show growth in vertebral height before and after vertebroplasty, measured at anterior border (an), medial (mi), and posterior border (po) of the vertebral body at right (image at left), middle (middle), and left (image at right) for both modalities. Compared to control subjects, postprocedural mean height of treated vertebrae increased significantly (p < 0.001) from 4% to 38% of initial height, after vertebroplasty for an overall increase of 0.1-1.5 cm, median value 0.16-0.27 cm. All images courtesy of Dr. Johannes Hierholzer. |
 |
In the treated patients, however, postprocedural mean height increased significantly (p < 0.001) between 4% and 38% of initial height after vertebroplasty (overall increase 0.1-1.5 cm, median value 0.16-0.27 cm). The greatest elevation was seen in the center of the vertebrae (0.1-1.3 cm), while the posterior wall, being less compressed initially, displayed only mild augmentation (0.1-0.9 cm). The anterior part of the vertebral body was augmented from 0.2-1.5 cm.
 |
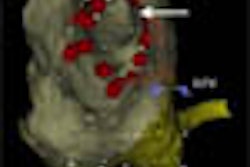
| Graphs show absolute changes in vertebral height before (left) and after (right) vertebroplasty, in centimeters (above), as well as the relative differences in height, expressed in centimeters (left) and percentage increase in height (below right). Links = left, rechts = right, vorn = anterior, mitte = middle, hinten = posterior. Charts courtesy of Dr. Johannes Hierholzer. |
 |
There is naturally more enhancement potential in the anterior and central parts of the vertebral body compared to the posterior border, Hierholzer said, and more potential enhancement in the thoracic and lumbar spine compared to thoracolumbar spine. "If you stratify the vertebral bodies, you will find in the thoracic spine there is a significant increase in height as compared to the thoracolumbar spine and the lumbar spine," he said. Vertebroplasty is most often performed in the thoracolumbar spine.
"And we would expect that if there is a great deal of compression we would have greater potential correcting that as compared to a fracture that is hardly compressed, which cannot be augmented, of course," Hierholzer said. The kyphotic angle was also reduced significantly (mean -3º) following treatment.
The effect of patient posture on the results was not analyzed but might be significant, Hierholzer said in response to a question from the audience. It remains unclear whether the augmentation is a result of the cement injection or rather the effect of patient posture during the procedure, he said.
"I would hypothesize that if we (were to) measure an erect lateral radiograph and then look at the form of vertebral body in posture ... we would probably see a degree of enhancement in height even without injecting cement," Hierholzer said.
By Eric Barnes
AuntMinnie.com staff writer
May 2, 2006
Related Reading
New fractures occur sooner in adjacent vertebrae following vertebroplasty, January 24, 2006
Vertebroplasty packs radiation punch, but cement injector can soften blow, December 5, 2005
Copyright © 2006 AuntMinnie.com