Rosai-Dorfman disease is an idiopathic proliferative disorder of the histiocytes in the lymph nodes. This benign disease is also known as sinus histiocytosis with massive lymphadenopathy. Rosai-Dorfman disease is most commonly found in the upper airway, subcutaneous tissues, and salivary glands.
The disease can infiltrate the breast, and imaging can help make the differential diagnosis between this disease and other breast disorders, according to a number of published reports. But even imaging has its pitfalls.
"The diagnosis of Rosai-Dorfman disease of the breast is difficult on imaging studies as it can simulate suspicious breast masses on mammography and can resemble neoplastic processes on ultrasound and CT," explained Dr. Minh Nguyen and colleagues in their paper on Rosai-Dorfman of the breast. "Tissue sampling is necessary. Thus, while rare, the medical community should be aware of this benign entity, which can mimic malignant lesions, both clinically and radiographically" (Journal of Women's Imaging, June 2005, Vol. 7:5, pp. 61-64).
Radiologists from the University of Texas M. D. Anderson Cancer Center in Houston reported on a 57-year-old woman who presented with an ill-defined mass in the left breast on screening mammogram. The latter exam showed a 1.5-cm, high-density mass with indistinct margins.
A subsequent ultrasound exam revealed an ill-defined, hypoechoic mass. A histopathological exam of a biopsy sample "revealed a polymorphous infiltrate of histiocytes … with round nuclei (that) expressed S-100 protein, characteristic of Rosai-Dorfman disease," wrote Dr. Cynthia Pham and colleagues (American Journal of Roentgenology, October 2005, Vol. 185:2, pp. 971-972).
 |
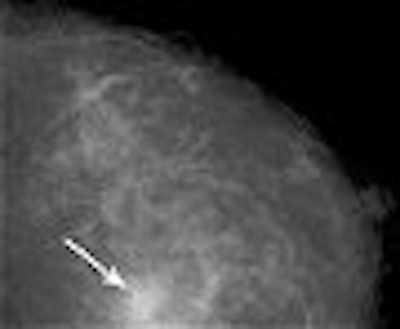
| Fifty-three-year-old woman with Rosai-Dorfman disease of the breast. Above, left breast craniocaudal mammogram shows 1.5-cm high-density mass with indistinct margins (arrow). Below, left breast longitudinal sonogram shows ill-defined, hyopechoic mass. Pham CB, Abruzzo LV, Cook E, Whitman GJ, Stephens TW, "Rosai-Dorfman Disease of the Breast" (AJR 2005;185:971-972). |
 |
The patient was ultimately diagnosed by ultrasound-guided needle core biopsy followed by stereotactic vacuum-assisted core biopsy, the authors stated, adding that surgery was unnecessary.
In a second case, Nguyen's group from Santa Clara Valley Medical Center in San Jose, CA, reported that a 54-year-old woman with a history of cervical carcinoma was undergoing her annual mammogram when a 1-cm rounded mass with lobulated and ill-defined margins was discovered. It was initially interpreted as suspicious for malignancy and given a BI-RADS 4. The patient had excisional biopsy and the histology was consistent with Rosai-Dorfman disease.
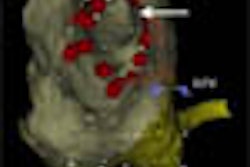
The scenario was nearly the same in a third report, although this time the authors used FDG-PET. Dr. Jian Yu and co-investigators from the University of Pennsylvania in Philadelphia dealt with a 58-year-old woman with a history of breast cancer. Postmastectomy, she underwent FDG-PET scans to evaluate for possible recurrence. The attenuation, noncorrected images demonstrated "intense activity in the neck and several foci of moderately increased FDG activity in the right hilum, mediastinum, and posterior lung," they wrote (Clinical Nuclear Medicine, March 2004, Vol. 29:3, pp. 209-210).
Of course surgical pathology did not identify any cancer cells and Rosai-Dorfman disease was the final diagnosis. The authors cautioned that "a variety of nonmalignant processes can result in increased FDG activity."
As Nguyen pointed out, tissue sampling is a must for a final Rosai-Dorman diagnosis and fine-needle aspiration (FNA) is one reliable option.
"The differential diagnosis of Rosai-Dorfman disease of the breast on FNA includes a variety of reactive and neoplastic lesions," explained Dr. Pascale Hummel and colleagues from the department of pathology at New York University Medical Center in New York City (Diagnostic Cytopathology, October 1999, Vol. 21:4, pp. 287-291).
They performed aspiration biopsy of the breast with a 25-gauge needle in a 52-year-old insulin-dependent diabetic woman. The aspiration biopsy smear of the mammary lesion revealed multiple characteristics including large, pale, polygonal histiocytes with at least one vesicular nucleus.
The authors stated that a hallmark of mammary Rosai-Dorfman disease is the histiocytes, as well as ample cytoplasm. "The atypia of the nuclei may suggest a malignant proliferation, and lymphophagocytosis can be interpreted as lymphocytes overlapping histiocytes and giant cells," they wrote.
A final Rosai-Dorfman disease diagnosis is simply not possible without some type of histological exam, agreed Dr. Cherie Kuzmiak and co-authors from the University of North Carolina at Chapel Hill.
Their imaging studies in a 30-year-old patient yielded little conclusive information -- a firm mass on physical exam, an irregular mass with ill-defined margins on mammography, an irregular mass with posterior shadowing on ultrasound, and an irregular soft-tissue mass on CT.
"Whereas the imaging findings may vary, the microscopic appearance of the … disease has distinct features," wrote Kuzmiak's group. "Other diseases may have a microscopic resemblance to Rosai-Dorfman disease; nevertheless, Rosai-Dorfman disease can be distinguished from other entities because of its cell populations, rare mitosis, and strongly positive staining for the S-100 protein" (AJR, June 2003, Vol. 180:6, pp. 1749-1742).
By Shalmali Pal
AuntMinnie.com staff writer
December 2, 2005
Related Reading
Scintimammography-SPECT valid as secondary test for ambiguous breast cancer, October 18, 2005
Lymph node involvement tied to recurrence of breast cancer, August 19, 2005
Copyright © 2005 AuntMinnie.com