The recent focus on rising CT radiation dose has some radiologists looking for alternative imaging tools. Some are wondering whether the solution could come from radiology's oldest modality -- radiography -- which is gaining renewed attention thanks to a trio of new digital technologies.
Digital tomosynthesis, computer-aided detection, and dual-energy imaging all have the potential to increase the sensitivity of digital radiography (DR) to the point where it becomes more competitive with CT. But all three tools also have significant drawbacks, and most radiologists are as yet reluctant to hold up DR as radiology's savior.
Still, should ongoing research pan out, DR with advanced imaging tools could enable radiologists to make more judicious use of CT while giving a new lease on life to good ol' x-ray.
Rising radiation dose
CT's rapid rise in use over the last few decades has come in large measure due to its clear superiority over standard analog radiography in terms of sensitivity and functionality. But that growth has come at a price -- a rapid increase in exposure to medical radiation among the U.S. population that has drawn the attention of everyone from the U.S. Food and Drug Administration (FDA) to Congress.
Solutions ranging from more efficient CT image acquisition to better physician education to reduce inappropriate scans are being implemented to reduce patient dose. Yet, the lowly x-ray has largely been overlooked as a possible diagnostic alternative to the more than 72 million CT scans that will be performed in the U.S. this year.
In fact, the 0.02-mSv dose that the FDA says is typical for an anterioposterior chest x-ray has become the unofficial benchmark that imaging critics and proponents use to underscore the potential dangers of much higher radiation from fluoroscopy, nuclear medicine, and CT procedures.
General radiography can't deliver the nearly surgical anatomic image quality possible with multidetector-row CT, but as industry observers note, the doses from general x-ray are low. It is inexpensive, and its versatility has sustained x-ray as the most frequently used imaging modality in radiology. It still accounts for about 60% of the procedures performed in a busy hospital imaging department.
In addition, three major technical developments promise to boost DR's diagnostic power for chest imaging:
|
||||||||||||||||||||||
- Dual-energy imaging: Digitally subtracts bone from lung soft tissue to reveal pulmonary nodules that would otherwise be hidden behind ribs or clavicles.
- Computer-aided detection (CAD): Serves as an inexpensive second reader, helping increase the diagnostic yield, especially for inexperienced radiologists.
- Digital tomosynthesis: Creates a sense of depth and volume for detecting pathology that is difficult to characterize with standard 2D radiography.
Part of DR's surge is due to the increased flexibility possible with the modality. The ability to integrate DR images into PACS and teleradiology systems enables the efficient transmission, presentation, and review of digital images anywhere within the healthcare enterprise and geographically beyond. As a result, use of traditional film-screen radiography is declining and the sale of DR units is increasing (see chart).
Though CT remains the modality of choice for many chest applications, researchers point to situations where each innovation could encourage clinicians to forego CT.
Dual-energy imaging
Dual-energy imaging takes advantage of the fact that different types of tissue have different responses to different x-ray energy levels. The technology delivers x-ray beams at two different energies to the same target, and via an energy subtraction process can be manipulated to either display exclusively bone or soft tissue.
The potential diagnostic advantages of digitally subtracting bone from soft tissue have been known since research conducted in the early 1990s. Dr. John H. M. Austin at Columbia University Medical Center in New York City, for example, showed that 81% of missed lung cancers were partially obscured by ribs and clavicles (Radiology, January 1992, Vol. 182:1, pp. 115-122).
 |
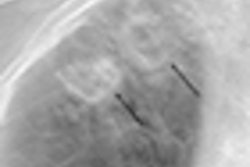
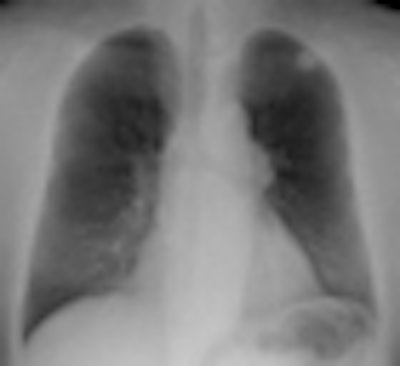
| Standard PA chest radiograph (left) shows a nodule in the left upper lobe (arrow), partly obscured by overlying bones. Dual-energy subtraction image (right) provides more complete bone subtraction, but requires specialized equipment. |
Dr. Reginald Munden, chairman of radiology for the University of Alabama at Birmingham (UAB) Health System, has found that CT is often avoided when dual-energy imaging determines that a suspicious mass is a calcified granuloma.
"If dual-energy indicates that, then I'm finished," Munden said in an interview. "We don't need to anguish over what that nodule is."
Munden also expressed confidence in dual-energy imaging for ruling out the presence of recurrent cancer for patients receiving routine follow-up imaging.
"If that dual-energy subtraction image is negative, then I'm pretty comfortable the results are actually negative," he said.
Dual-energy imaging can be performed on either of the two major digital x-ray technologies, DR and computed radiography (CR). For energy subtraction on its ClearView-ES CR system, Fujifilm Medical Systems USA of Stamford, CT, used two dual-sided photostimulable phosphor detectors separated by a copper filter to differentiate between low-energy 60-80 kVp photons for soft tissue and high-energy 100-150 kVp photons that characterize bone.
The system's front plate detects high- and low-energy photons, while the back plate detects only high-energy photons. Weighted subtraction software processes the data to produce separate bone, soft tissue, and composite images for interpretation.
Copper filtration was not possible, however, when Fuji switched to amorphous selenium flat-panel detectors for its next-generation AcSelerate DR system. The work-in-progress energy subtraction system for that product, introduced at the 2009 RSNA conference, uses a dual-exposure approach.
Fuji's engineers are banking on the high detective quantum efficiency (DQE) of selenium detectors to shift to a dual-exposure approach without increased dosage, said Penny Maier, director of marketing at Fuji.
On its DR systems, GE Healthcare of Chalfont St. Giles, U.K., employs a two-shot dual-energy technique that uses rapid kilovolt (kV) switching during high- and low-energy acquisitions captured by a single digital detector to subtract bone for the three images. GE touts its flat-panel amorphous silicon detector as a key to acquiring high- and low-energy images in quick succession. The two exposures are separated by less than 200 msec to avoid motion artifacts, but because two acquisitions are required, the total radiation to the patient is slightly more than a standard radiograph.
In terms of radiation dosage, there is typically no difference between the exposure from a 400-speed film-screen radiograph and flat-panel digital radiography, according to J. Anthony Seibert, Ph.D., a professor of radiology physics at the University of California, Davis. His calculations suggest that a chest x-ray exposes a patient to about 140 times less radiation than a low-dose chest CT. Computed radiography, which records images on phosphor plates before digitization, requires about twice the effective dose of film or DR, he wrote in an e-mail response to questions.
Researchers disagree about the effect of dual-energy radiography on radiation exposure, however. The effective dose for dual-energy digital radiology for posteroanterior (PA) and lateral views is about 0.1 mSv, or 30% to 50% more radiation than from standard chest DR, according to Seibert.
Other researchers have reported that dual-energy imaging generally involves about 14% more radiation exposure during the acquisition of PA and lateral chest views than conventional imaging. Dr. Heber MacMahon, section chief of thoracic radiology at the University of Chicago Medical Center, argues that the percentage dose increase in this context is insubstantial, especially for adult patients, and should not affect clinical decision-making. If the clinician is concerned about dual energy's higher dose, it can be reduced by adjusting machine settings for the lateral view, he said.
Dual-energy effectiveness
How effective is dual-energy imaging in a clinical environment? In one of only a few efficacy trials of dual-energy imaging, the University of Chicago group demonstrated in 2008 that it can help radiologists detect small lung cancers that were previously missed with conventional radiography (American Journal of Roentgenology, April 2008, Vol. 190:4, pp. 886-891).
Practical experience with dual-energy imaging has led Munden at UAB to expand its use for more types of chest applications, such as visualizing catheters and lines. Inexperienced radiologists benefit most from the ability to view separate bone and soft-tissue images, but even fellowship-trained thoracic radiologists improve their reading accuracy, he said.
The cost and possible clinical inefficiency of dual-energy imaging have limited its popularity, however. Dual-energy capabilities add $20,000 to $30,000 to the purchase price of a standard DR system. Though some radiologists believe dual-energy imaging speeds interpretation, others think the extra images add to reading time.
MacMahon described situations in which dual-energy imaging could rule out the need for CT, but he cautioned that it could never serve as a substitute. CT detects much smaller abnormalities than dual-energy subtraction and characterizes them more accurately.
There is no question that CT will be ordered as the next test for patients after positive findings suspicious for cancer are found on digital chest x-ray, according to MacMahon.
"As long as we are going to be doing chest x-rays, if we can increase their yield by just a few percentage points, that could have a significant impact on healthcare and, in some cases, could detect cancers earlier or rule out the need for CT because we can have higher confidence," he said.
In part 2 of our report on new DR technologies, we address computer-aided detection and digital tomosynthesis.
By James Brice
AuntMinnie.com contributing writer
March 24, 2010
Related Reading
Low-dose tomo beats chest DR for TB evaluations, March 19, 2010
Virtual dual-energy DR improves lung lesion detection, February 10, 2010
Rads prefer dual-energy x-ray over standard DR in lung, January 29, 2009
Adding CsI-based dual-energy imaging doesn't improve lung nodule detection, December 26, 2008
Dual-energy digital x-ray still looking for acceptance, February 22, 2007
Copyright © 2010 AuntMinnie.com