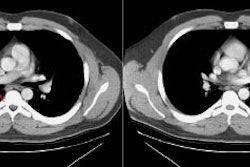
Metastasis:
View cases of lung metastases
General:
Metastases are the most common neoplasms of the lungs. The most
common tumors to
metastasize to the lungs include breast, colon, pancreatic,
gastric, renal, and head and
neck cancers. Melanoma also has a propensity for lung metastases.
Tumors which commonly
have pulmonary mets at the time of diagnosis include renal cell
carcinoma, choriocarcinoma,
Wilm's tumor, Ewing's and osteosarcomas. Cavitation is seen only
infrequently with
metastatic lesions (4%)- most commonly head and neck squamous cell
carcinoma metsatases from the larynx, pharynx, or esophagus, but
also from the cervix [5]. These sites account for up to 2/3's of
cavitary metastases [5]. Adenocarcinomas of the colon or rectum
can also produce cavitary metastases [5]. Metastatic sarcomas and
lymphoma can also present as cavitary nodules. Occasionally,
sarcomas may cavitate with a very thin wall and may mimic
pneumatoceles. The overwhelming majority of lung metastases
present as multiple pulmonary
nodules (90-97%). At autopsy, nearly 60% of metastatic lesions to
the lungs are found to
be smaller than 5 mm, and more than 80% are either subpleural or
in the outer one-third of
the lung. The presence of a solitary metastasis to the lung is
uncommon, and a solitary
pulmonary nodule in a patient with a known underlying malignancy
most likely represents a
second primary, rather than a metastatic lesion. Tumors that more
commonly present with a solitary pulmonary metastasis include
primary tumors of the colon and kidney, melanoma, and sarcoma [4].
Endobronchial metastases are rare (2-5%
of patients at autopsy) and the proximal airways are most commonly
involved [4]. Renal cell carcinoma is the most common tumor to
metastasize to the airways, but other lesions with the potential
for airway involvement include melanoma, lymphoma, and tumors of
the breast, larynx, thyroid, and colon [4].
CT-guided 125I brachytherapy may hold promise for the
treatment of pulmonary metastases in patients with pulmonary
metastases from recurrent colorectal cancer [5].
Osteosarcoma:
The most common location for primary osteosarcoma is about the knee (50%), followed by the proximal humerus (15%). Common sites for metastases are the lungs and bones. Pulmonary metastases are common in osteosarcoma- occurring in more than 85% of cases. Computed tomography is regarded as the imaging agent of choice for detecting metastatic lesions in these patients. Metastatic lesions are typically mulitple, well circumscribed, bilateral, ossified or non-ossified nodules. Nodules may be unilateral in up to 35% of cases. In about 5% of cases, spontaneous pneumothorax develops in association with subpleural metastases [1]. Scinitgraphy is much less sensitive than CT in the detection of pulmonary metastases (with single headed tomography detecting only 8% of lesions identified by CT in one series [2]). Although tracer uptake within a pulmonary lesion is very specific for a metastatic focus of osteosarcoma, the additional cost of tomographic images to detect lung lesions is difficult to justify, given its lack of sensitivity compared to CT.
(1) AJR 1997; Thoracic involvement from osteosarcoma: typical and atypical CT manifestations. 168: 347-349 (No abstract available)
(2) AJR 1984; Sep 143(3): 519-523
(3) AJR 1998; Pevarski DJ, et al. The
usefullness of bone
scintigraphy with SPECT images for detection of pulmonary
metastases from osteosarcoma.
170: 319-322
(4) Radiology 2016; Wang G, et al. Feasibility and clinical value
of CT-guided 125I brachytherapy for bilateral lung
recurrences from colorectal carcinoma. 278: 897-905
(4) Radiol Clin N Am 2005; Aquino SL. Imaging metastatic disease to the thorax. 43: 481-495
(5) AJR 1990; Alexander PW, et al. Cavitary pulmonary metastases in transitional cell carcinoma of the urinary bladder. 154: 493-494