Tc99m Pyrophosphate Imaging of Acute Myocardial Infarction
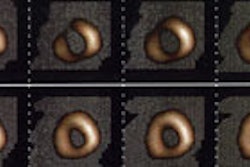
Tc-Pyrophosphate has been used for detection of myocardial infarction. It is used less commonly today because of the improved enzymatic detection methods for MI. The typical dose is 15-20mCi. Pyrophosphate binds to mitochondrial calcium complexes and proteins in the area of necrotic myocardium. Myocardial uptake of the tracer is often seen within 10 to 12 hours after infarction and becomes maximal between 24 to 72 hours post event. The scan may remain very positive for up to 6 days. The activity begins to fade by 7 days and the exam is usually negative by 10-14 days post event. In large infarcts, there may be a "doughnut" appearance to the activity as less tracer will reach the central necrotic zone. Planar imaging detects acute transmural infarctions with a sensitivity of at least 90% and a specificity of 70%. SPECT imaging can improve detection of non-Q wave MI's and improve the specificity of the exam to about 80%. Owing to the limited resolution of SPECT systems, infarcts that are smaller than 10 gm (equivalent to about 10ml) are difficult to detect.
Grading: Must be at least Grade 2 to be considered positive
0: No increase
1: Faint increase activity
2: Equal to ribs, but less than sternum
3: Equal to sternum
4: Greater than sternum
Positive Exam can be due to:
- Acute MI
- Myocardial contusion/Resusitation
- Cardiomyopathy
- Unstable Angina
- Cardioversion (Diffuse uptake)
- Amyloid heart (Diffuse intense uptake)
- Myocarditis/Pericarditis
- Valvular calcification- usually very focal
A persistently positive scan (over months) indicates continued myocardial necrosis (ongoing ischemic damage). Dystrophic calcification may contribute to the uptake, but the finding is generally associated with a worse prognosis. This finding has also been decribed with the presence of a mural thrombus or ventricular aneurysm.