NEW ORLEANS - Epileptic patients who exhibit a resistance to anti-seizure medication may be helped by surgery. However, the success of an operation, such as anterior temporal lobectomy, depends on the localization results of PET and SPECT imaging. At the 2003 Society of Nuclear Medicine meeting, Dr. Christopher Rowe from Austin Hospital in Melbourne, Australia discussed the role of imaging in preoperative planning for patients with partial seizures.
"Medically refractory, or medically resistant epilepsy, affects 0.1 to 0.5 % of the general population. Most refractory epilepsy is focal in origin, and most focal epilepsy is temporal lobe epilepsy (TLE). In fact, 50% of patients with TLE cannot be controlled completely with medication," Rowe said during a categorical session on Saturday, adding that anterior temporal lobectomy provides seizure freedom in 70% or more of patients with intractable TLE.
Resection elsewhere in the brain is less successful and more risky, Rowe said in reference to another surgical option, resection of the extratemporal foci, which renders only 40-50% of patients free of seizures.
The presurgical evaluation of epilepsy patients is a multiphase process, involving such noninvasive tests as interictal EEG, neuropsychology assessments of verbal and non-verbal memory, PET and MR, and interictal SPECT.
"Most patients only require non-invasive workup these days, but some patients do require invasive EEG studies, usually when the non-invasive modalities give contradictory or inconsistent results," Rowe said. "The problem with (EEG studies) using subdural electrodes is that you can’t cover the whole brain. You have to have a fairly good idea where the seizures are coming from. Advances in imaging have dramatically reduced the need or invasive electrodes studies."
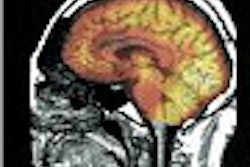
PET for hypometabolism
PET scans, with tracers such as FDG or ammonia, are useful for demonstrating hypoperfusion and hypometabolism involving the temporal lobe, which contains the seizure focus. While the degree of hypometabolism can vary greatly from person to person, the condition is present in the affected lobe in more than 80% of patients with refractory TLE.
A 10% or greater relative reduction in metabolism in the left temporal lobe on preoperative FDG-PET is associated with a lower risk of postsurgical, verbal memory impairment, Rowe said. In addition, for TLE patients with normal MR results, PET scans will reveal temporal lobe hypometabolism in 60% of the cases.
Rowe cited an example of how the PET scan drastically altered the course of surgery in one of his patients. "Before the PET scan, the surgeon was sharpening his scalpel for a left temporal lobectomy," Rowe said. The MR results showed severe hippocampal sclerosis on the left while the psychology tests showed verbal memory impairment.
"But the PET showed quite profound right temporal hypometabolism. Backing up the PET finding, the interictal EEG showed spiking a bit more on the right than the left." Further invasive EEG testing showed that the majority of the seizures were coming from the right, not the left, lobe, Rowe said.
"Now if this patient had had a left temporal lobectomy, it would have been a complete disaster. Not only would they have continued to have seizures, but their entire memory function would have been dependent on this one very dysfunctional right temporal lobe," he said.
Rowe added that his group is currently working with 11Cflumazenil PET (FMZ-PET) in order to study the pathogenesis of epilepsy in the benzodiazepine receptor. Unlike the hypometabolic changes seen on FDG-PET studies, FMZ-PET reveals tracer binding in the mesial temporal lobe, which may make it a more sensitive test for patients with TLE arising from the amygdala/hippocampal regions.
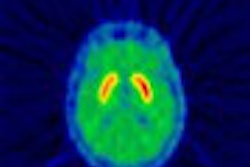
SPECT during seizures
"SPECT can be used to show the cerebral blood flow both between seizures (interictal) and during the seizures (ictal). It can be done with Ceretec (99mTC exametazine) and Neurolite (99mTC ECD). Both have rapid brain intake and do not wash out," Rowe said.
Between seizures, blood flow metabolism is reduced in the area of seizure focus. During seizure, blood flow increases dramatically at the seizure focus. Immediately following a seizure, blood flow is profoundly decreased, Rowe explained.
Most complex partial seizures last 40-90 seconds. Tracer injection is generally done within 60 seconds of seizure onset, and is performed by an EEG technologist. In the case of extratemporal foci, radiotracer injection must be done quickly in order to truly catch the seizure foci, Rowe said.
"(We had) a patient with asymmetrical seizures that would last about 28 seconds. On MRI, there was a highly suggestive lesion, but we just wanted to try and prove that prior to surgery. In the first study, ictal and post-ictal, we injected 73 seconds after seizure onset, and didn’t show anything. We tried it again, this time within 33 seconds, and there was the hyperperfusion correlating very nicely (with the MR results)," Rowe said.
Previous studies have showed that ictal SPECT correctly identifies the seizure focus 90% of the time. For post-ictal SPECT with the injection given an average of four minutes after seizure onset, the localization rate is 70%. Interictal SPECT is more useful as a comparison tool to the ictal SPECT scans.
"Most centers use subtraction studies," Rowe said. "Subtraction can be useful when you have bilateral temporal hyperperfusion, highlighting which side has the greatest hyperperfusion." In general, the size of greatest hyperfusion correlates with seizure focus, he added. Subtraction SPECT studies, with co-registration on MRI, also can aid the neurosurgeon in preoperative mapping.
However, ictal SPECT may be misleading when seizures arise from the posterior parts of the brain, Rowe said. In patients with occipital lobe epilepsy, ictal SPECT will show temporal lobe hyperperfusion of greater degree and duration than in the true area of focus.
"In summary, PET and ictal SPECT are the most sensitive imaging modalities for seizure localization. PET is a good predictor of surgical success," he said. "It may have an important role in predicting memory function after surgery although more studies are needed. Interpretation of ictal SPECT requires knowledge of injection timing, MRI findings, and clinical and EEG findings. Neuroreceptor imaging holds promise for further improvement in noninvasive seizure focus detection."
By Shalmali PalAuntMinnie.com staff writer
June 22, 2003
Copyright © 2003 AuntMinnie.com