Technique Prior
to performing a percutaneous transthoracic needle biopsy, patient consent must be
obtained. As part of the preliminary evaluation, patients should have a prothrombin time
(PT) and platelet count performed within two weeks of the procedure. Anticoagulation and
antiplatelet medications should ideally be discontinued for 7 days. Patients with a single
lung (contralateral pneumonectomy) are not generally considered candidates for
percutaneous biopsy procedures. Some relative contraindications to transthoracic needle
biopsy include an inability of the patient to cooperate (i.e., cannot hold their breath or
cannot be positioned for the procedure), underlying coagulopathy (PT > 15 sec,
international normalized ratio > 1.3, or platelet count below 50,000/cm3), severe COPD
(i.e., patients who cannot tolerate even a small pneumothorax), patient on mechanical
ventilation (increases risk for pneumothorax and brochovenous fistula [91]), bullae in the
vicinity of the the lesion to be biopsied, a vascular lesion (AVM or aneurysm), and
pulmonary artery hypertension [85]. Aspirin use or chronic renal failure can cause
platelet dysfunction not reflected in clotting profiles. Some authors [91] consider the
previously described conditions to be contraindications to transthoracic biopsy --
individual physicians should use sound clinical judgment and discuss the case with the
appropriate specialists when making decisions regarding complicated patients.
An intravenous line, blood pressure monitor,
electrocardiogram leads, and an oxygen saturation monitor should be placed. The biopsy
room should be equipped with oxygen, suction, oral and nasal airways, an Ambu-bag, a
Pleur-evac device [95], and a crash cart. After lesion localization, the biopsy needle can
be introduced alone, or as a coaxial system. The needle should be passed over the rib (not
under) to avoid the neurovascular bundle. Fissures should be avoided because their
transgression leads to three visceral pleural punctures rather than one. The use of thin
(1-2 mm) localizing images may be very helpful in detecting blebs not seen on thicker
section images, particularly in patients with underlying emphysema [91]. Specimens should
be obtained during suspended respiration. Cytopathology support during the procedure is
essential. In addition to aspiration samples, some centers perform core biopsies with a
cutting needle.
Results Percutaneous
needle biopsy can be of tremendous value in patient diagnosis. With the use of 20 to 22
gauge aspiration needles and expert cytopathology, sensitivities of 90 to 95% can be
expected in the diagnosis of primary intrathoracic malignancy. The ability to distinguish
non-small-cell from small-cell carcinoma approaches 100%. The accuracy of percutaneous
biopsy, however, is affected by the size of the lesion, and decreasing accuracy is found
to be associated with smaller lesions. Unfortunately, reliability in the diagnosis of
benign lesions is not as high with a very variable yield of only 16 to 68% [85]. Often, a
core biopsy will be necessary to confirm that a lesion is benign. An automatic biopsy
device with a short throw (1 cm) can significantly increase the diagnostic accuracy for
benign lesions, while maintaining acceptable complication rates [86,93,102]. Up to 76% of
benign lesions can be accurately identified with the use of a core specimen [93]. Cutting
guns should never be used in a chronically infected cavity or in regions of bronchiectasis
that might be associated with substantial bronchial artery hypertrophy as there is an
increased risk for hemorrhage [91].
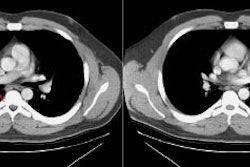
Examples of percutaneous biopsies:
Example 1: In this patient with a superior sulcus tumor,
CT-guided biopsy permits avoidance of vascular structures.
NOTE: To load a higher resolution
view, simply click directly on the image below.
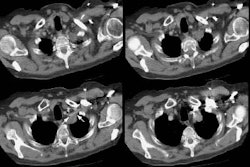
Example 2: Peripheral lesions are easily biopsied with the
aid of computed tomography. Bronchoscopic biopsy is generally unsuccessful when lesions
are this peripheral.
Complications:
1. Pneumothorax: The incidence of
pneumothorax following CT-guided transthoracic needle biopsy is generally reported to be
between 20 to 30% and is felt to be somewhat higher than the incidence of pneumothorax
following fluoroscopic-guided biopsy. Most pneumothoraces occur during or within the first
hour after biopsy. Only about 2% of pneumothoraces will be first detected on four hour
post-procedure films. Factors which are associated with an increased risk of pneumothorax
include emphysematous changes within the lungs, coughing or breathing during the
procedure, increased lesion depth (when traversing aerated lung), smaller lesion size,
multiple pleural punctures, using cutting needles or biopsy guns to obtain core biopsies,
and positive pressure ventilation. Pneumothorax is much less likely to occur if the lesion
can be biopsied without traversing aerated lung [115]. The use of a coaxial technique
permits multiple needle passes from a single pleural puncture. The use of spring-loaded
biopsy guns should be reserved for large lesions with a diameter exceeding the throw of
the needle (usually 20-23 mm), or for those which have a broad pleural attachment [85-89].
Whether to treat the pneumothorax with a chest tube depends on the patient's pulmonary
reserve, the patient's symptoms (dyspnea), or whether the pneumothorax is enlarging over
time. Chest tube drainage of post-procedure pneumothorax is required for between 2% to 14%
of cases [87]. The severity of the pneumothorax and the need for chest tube placement
appear to be correlated with the severity of underlying obstructive airway disease
[88].
In an attempt to reduce the prevalence of pneumothorax
following the procedure, several maneuvers have been suggested. Positioning the patient so
that the biopsy side is in the dependent position is perhaps the most successful. It is
postulated that this maneuver reduces both alveolar size and the differential of alveolar
and pleural pressure. These changes favor the development of dependent atelectasis and
close approximation of the parietal and visceral pleura. The administration of oxygen
(100% at 2-3 L/min) to patients before, during, and following the procedure may also be
useful. The theoretic basis for this is that should a pneumothorax develop while the
patient is breathing high concentrations of oxygen, the air in the pleural space would
also be oxygen rich. A pneumothorax will decrease more rapidly in this setting since
oxygen is resorbed into blood faster than air. Aspiration of large immediate
post-procedure pneumothoraces using a standard 18 g IV catheter may decrease the need for
chest tube placement. In one study of patients with large post-procedure pneumothoraces,
immediate aspiration of the air avoided the need for chest tube placement in 70% of these
patients [89]. Patients who develop clinically important pneumothoraces have also been
managed as outpatients with short-term small caliber chest tubes [90].
2. Hemorrhage: The incidence of hemorrhage following
transthoracic biopsy ranges from 1 to 10%- it is the second most common complication of
transthoracic biopsy. The use of a biopsy gun is associated with an increased risk for
hemorrhage
[91]. Hemorrhage is almost always self-limiting [85]. The
likelihood of hemorrhage is greater for vascular lesions (such as renal-cell carcinoma),
patients with an underlying bleeding diathesis, patients with pulmonary arterial or venous
hypertension, and with the use of larger cutting needles. Patients with hemorrhage should
be placed biopsy side down to decrease the risk of blood being carryied into the opposite
lung. During parasternal biopsy procedures, care should be taken to avoid the internal
mammary vessels which lie about 1.25 cm lateral to the lateral margin of the
sternum.
3. Systemic air embolization: This is a very rare
complication of the procedure. Air embolism most likely occurs due to air entering the
pulmonary vein either directly from the needle open to the atmosphere or from a broncho-
or alveolovenous fistula induced during placement of the needle. Factors which increase
airway pressure result in an increased risk for air embolism including coughing, the deep
inspiration which precedes coughing, and positive pressure ventilation. Biopsy guns may
also increase the risk for air embolism [91]. Complications of air embolism include
myocardial infarction, stroke, or death. As little as 0.5 ml of air is sufficient to
induce coronary artery ischemia and fatal arrhythmias. Treatment consists of placing the
patient in a left lateral decubitus position (to prevent air within the left atrium from
embolizing systemically) or Trendelenberg position (to keep air out of the cerebral
circulation). Ventilatory support with 100% oxygen should be administered to promote
resorption of air bubbles. Transfer to a hyerbaric chamber may be necessary. [85]
Example of air embolism:
In this case, a percutaneous biopsy of a right hilar mass
was attempted. The chest CT demonstrates that the biopsy needle had entered into the right
pulmonary vein (yellow arrow). During the biopsy, the patient experienced a generalized
seizure. A head CT scan was obtained and revealed air in the venous sinus (black
arrow).
NOTE: To load a higher resolution view, simply click directly on either image
below.
4. Malignant seeding of the biopsy tract: Although seeding
may occur, it is an extremely rare complication (0.012%). The risk malignant seeding of
the biopsy track is random -- no definite risk factors have been described [92].
5. Death: The mortality rate from
transthoracic needle biopsy is 0.02% [85]
Post-biopsy Management:
Some centers obtain post-biopsy chest
radiographs immediately following the procedure, while others delay this exam for one hour
to avoid straining associated with rising from a recumbent to a seated or standing
position. Selected CT images following the procedure can also be used to evaluate for the
presence of a pneumothorax. The biopsy site should be placed in a dependent position
following withdrawal of the biopsy needle. This maneuver decreases alveolar volume
adjacent to the puncture site, uses the weight of the lung to help tamponade the puncture,
and raises intrapleural pressure thereby decreasing the amount of air leak. An additional
benefit of this position is the prevention of transbronchial spread of hemorrhage that may
complicate the procedure. The use of a blood patch has been described, but has not been
demonstrated to be of significant value. Patients should be monitored with vital signs,
breath sounds, and oxygen saturations every 15 minutes for one hour and every 30 minutes
thereafter. Patients should remain in the biopsy site dependent position for at least 2
hours. Patients that have no pneumothorax following the procedure and at 4 hours post
biopsy can be discharged home. Patients should be instructed to avoid straining and all
but mild physical exertion until the following day. Patients should be instructed to
proceed immediately to an emergency room for any pleuritic chest pain, hemoptysis, or
shortness of breath. [85]
Most pneumothoraces requiring chest tube drainage are
detected within one hour of the biopsy. If a small or asymptomatic pneumothorax is present
post-procedure CXR's should be obtained at 2 and 4 hours. If the pneumothorax remains
stable and the patient remains asymptomatic, they may be released. If the pneumothorax is
enlarging (15 to 35% pneumothorax- depending on the patients respiratory status) or
becomes symptomatic, an 8 french catheter with a hollow inner trocar should be placed in
the lung apex over the second intercostal space in the midclavicular line. The air in the
pleural space should be aspirated and the catheter attached to a Heimlich valve or
Pleur-evac system. [85]