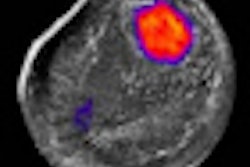
Sonoelastography can predict before surgery whether women with ductal carcinoma in situ (DCIS) have an invasive form of the disease, according to a study by Korean researchers presented at the recent RSNA meeting in Chicago.
In a study of 103 nonpalpable DCIS lesions diagnosed on core-needle biopsy, a team from Seoul National University Hospital in South Korea found that a sonoelastography elasticity score of 1 predicted the absence of an invasive component of DCIS in 100% of cases, while a score of 4 or 5 accurately forecasted an invasive component in 47.4% of cases.
"Sonoelastography stiffness is an independent predictor of invasion in DCIS lesions [found] at core biopsy," said Nariya Cho, MD.
DCIS diagnosed at core-needle biopsy is underestimated in 8% to 42% of cases in which the lesions are later found to be invasive and require further axillary lymph node sampling. And women with a high risk of invasive cancer need to have their axillary lymph node sampling planned preoperatively, Cho said.
As a result, the researchers sought to retrospectively evaluate the preoperative factors associated with why DCIS cases are upgraded to invasive cancers, focusing on the usefulness of sonoelastography in patients with an ultrasound-guided core-needle biopsy diagnosis of nonpalpable DCIS.
They reviewed the records of 3,510 consecutive women with 3,300 breast lesions who had undergone ultrasound-guided core biopsy and sonoelastography between June 2006 and May 2009. Histologic analysis found DCIS in 117 patients, but 15 were excluded from the study due to an unavailability of surgical histology.
The remaining 102 women (mean age, 50) had a total of 103 DCIS lesions (mean, 15 mm; range, 4-70 mm). All patients received sonoelastography and surgery after ultrasound-guided needle localization. The mean interval between ultrasound-guided core-needle biopsy and surgery was 31 days. Histopathology diagnosis was made by a combination of core-needle biopsy and surgical excision.
For data acquisition, one of five radiologists with three to seven years of experience in breast ultrasound performed B-mode ultrasound and sonoelastography on the patients and saved the cine clips in .avi format. Ultrasound-guided 11-gauge vacuum-assisted biopsy or 14-gauge automated core biopsy was then performed.
After reviewing the video clips in random order and without access to the histologic results, two other radiologists provided their B-mode ultrasound findings and then elasticity scores (from 1 to 5) based on the degree of lesion stiffness.
To determine the independent preoperative predicting factors of invasive cancer, the researchers utilized Fisher's exact test for univariate analysis and a multivariable logistic regression model. Factors such as lesion type, lesion size, biopsy method, nuclear grade, and the presence of comedonecrosis were analyzed.
The researchers found that the elasticity score was the only independent feature for predicting the presence of an invasive component. Upgrade rates were as follows:
|
"Lesions with a higher elasticity score tended to have more invasive components," Cho said.
The researchers did not find any difference in upgrade rates based on lesion type, lesion size, biopsy method, nuclear grade, comedonecrosis, and B-mode ultrasound findings.
By Erik L. Ridley
AuntMinnie.com staff writer
December 13, 2010
Related Reading
New elastography technique helps characterize breast lesions, June 16, 2010
Breast elastography gets high sensitivity marks in 7-year study, November 11, 2009
Elastography shines in assessing breast lesions, April 29, 2009
Ultrasound elastography shows potential in thyroid nodules, February 11, 2009
Ultrasound elastography shows strength for diagnosing rotator cuff tears, January 15, 2009
Copyright © 2010 AuntMinnie.com