A pilot study done earlier this year at the Cleveland Clinic Foundation in Ohio found that ultrasound could accurately detect the placement of endotracheal tubes during intubation for surgery. The patients in this test were adults without any airway complications (Annals of Emergency Medicine, January 2007, Vol. 49:1, pp. 75-80).
Anesthesiologists from France raised the stakes by evaluating sonography for tube placement in pediatric patients with difficult airways. They presented their results last week at the American Society for Anesthesiologists (ASA) meeting in San Francisco.
"Difficult airway management is a challenging situation in pediatric anesthesia," wrote Dr. Bruno Marciniak and colleagues, from the Centre Hospitalier Régional at the Universitaire de Lille in Lille, France, in one of two posters. "Glottis visualization is not always possible, and final confirmation of the tracheal tube is generally realized by clinical assessment or end-tidal capnography." But end-tidal capnography does not offer real-time results and requires insufflations, they added.
 |
| All images courtesy of Dr. Bruno Marciniak. |
For the first prospective study, the researchers enrolled 11 children (mean age of 28 months) who were scheduled for surgery and suspected to have difficulties with intubation. After induction of anesthesia, a 5-10 MHz linear transducer on a Titan ultrasound scanner (SonoSite, Bothell, WA) was placed transversely on the anterior neck just superior to the suprasternal notch. Direct laryngoscopy was performed and tracheal intubation took place. In instances of poor glottis visualization, tracheal catheterization was used. Tube placement confirmation was evaluated by ultrasound, auscultation, and end-tidal capnography.
According to the results, tracheal intubation was successful on the first attempt in seven cases. In the other four cases, intubation was successful on the second attempt or tracheal catheterization was required. One esophageal intubation occurred but it was immediately visualized on ultrasound. In all cases, tracheal tube placement was confirmed by sonography before end-tidal capnography.
Ultrasound's accuracy "in determining tube position seems to be an excellent and faster than any other method," the authors concluded.
In an interview with AuntMinnie.com, Marciniak said that imagers at his institution were initially hesitant about anesthesiologists using ultrasound in this setting, but grew more comfortable with it over time as it allowed them to devote more of their energy to reading films. In addition, radiologists at the clinic are consulted when imaging equipment is purchased by other departments, he said.
 |
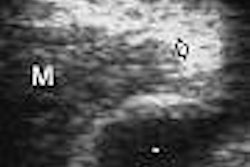
| Ultrasound confirmed the trachea (left) and the glottic plan (right). |
In the second study, Marciniak's group had 30 children (mean age of 48 months) scheduled for surgery under general anesthesia, although patients who met the criteria for difficult intubation were excluded. The same ultrasound placement as the previous study was used, and the probe was moved on the thorax and under the clavicle.
According to the results, the trachea was always identified on sonography by the tracheal rings. Also, the glottic plan was characterized by the visualization of the vocal cords, which moved during respiration. Finally, tracheal intubation provided enhanced shadowing posterior to the tracheal ring.
 |
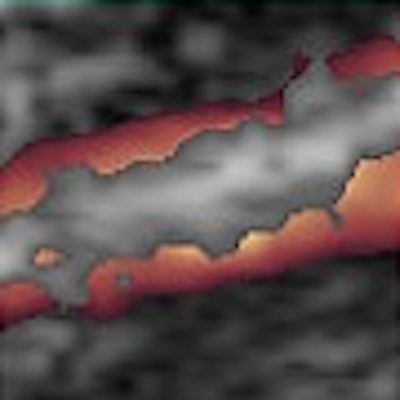
| Posterior shadowing indicates tracheal intubation (left). Sliding sign confirms tube position (right). |
While confirmation of the tube position was obtained in all cases by the sliding lung sign, the final visualization of the tube in the trachea was not always easy, the group stated, adding that the culprit was most likely interference between the echogenic characteristics of the tracheal ring and the tube. Doppler ultrasound may be one solution to improving tube visualization, Marciniak said.
As with sonography in general, successful visualization of the tube is operator-dependent. However, Marciniak told AuntMinnie.com that the learning curve for ultrasound-based tube visualization is quite low because it does not require as much technical precision as a diagnostic ultrasound.
By Shalmali Pal
AuntMinnie.com staff writer
October 29, 2007
Related Reading
Thoracic Imaging, July 2, 2007
3D PET/CT demonstrates virtual vigor, July 27, 2006
Copyright © 2007 AuntMinnie.com