Two new cardiac MR techniques reported in two studies in the June American Journal of Roentgenology may increase the modality's flexibility for assessing myocardial infarction (MI).
First, a study from the Netherlands offered clinical validation for free-breathing cardiac MR for MI assessment. The technique sidesteps the difficulty for some patients of performing long breath-holds during MR scans.
In a second study, from Ludwig-Maximilian University in Grosshadern, Germany, researchers evaluated myocardial viability on a 3-tesla MRI scanner, significantly reducing acquisition time and enabling shorter breath-holds.
The extent of viable myocardium in patients with ischemic cardiomyopathy has for years been understood as key to understanding long-term prognosis after coronary artery bypass grafting. MRI's higher spatial resolution compared to SPECT often makes it the preferred modality for assessing myocardial viability
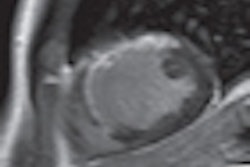
"In particular, the assessment of myocardial infarction using delayed-enhancement MRI is now routinely used for predicting recovery of left ventricle function after revascularization therapy," wrote Dr. Harrie van den Bosch from Catharina Hospital in Eindhoven, Netherlands, and colleagues. "Delayed-enhancement MRI provides the opportunity to evaluate the transmural extent of infarcted myocardium with superior spatial resolution compared with nuclear medicine techniques" (AJR, June 2009, Vol. 192:6, pp. W277-W281).
Free-breathing MRI technique
Among the validated techniques for delayed-enhancement MRI are breath-hold approaches using a segmented 2D fast low-angle shot inversion-recovery sequence and a rapid 3D inversion-recovery acquisition.
However, the 2D approach comes with long acquisition times encompassing 10 to 16 breath-holds of at least 10 heartbeats to cover the left ventricle in the short-axis orientation. Inability to perform adequate breath-holding and image misregistration can produce suboptimal results, using the 2D approach, van den Bosch and colleagues wrote.
On the other hand, the 3D technique has the advantage of imaging the entire heart in a single breath-hold. However, the 3D approach requires a breath-hold time of more than 20 seconds, a feat not all patients are able to perform.
"Therefore, it would be clinically desirable to have a delayed-enhancement MRI technique available that is not dependent on the ability of patients to hold their breath repetitively or for relatively long periods of time," the authors wrote.
To that end, the use of a 2D single-shot inversion-recovery steady-state free procession (SSFP) delayed-enhancement MRI sequence acquired during a single breath-hold has been reported for myocardial viability imaging. The fast delayed-enhancement MRI sequence is combined with respiratory triggering using a respiratory belt that allows the acquisition of delayed-enhancement MR images during free breathing, they wrote.
The researchers compared the technique with the accepted 3D breath-holding technique in a group of 32 patients (25 men, seven women; mean age, 68 years; age range, 39-84 years) with suspected chronic MI who underwent breath-hold gradient-echo 3D inversion-recovery delayed-enhancement MRI and free-breathing respiratory-triggered 2D inversion-recovery delayed-enhancement MRI of the heart (scanning time, 50-80 sec).
All images were obtained on a 1.5-tesla Achieva MRI scanner (release 10.3, Philips Healthcare, Andover, MA) with master gradients (maximum amplitude, 30 mtesla/m) and a dedicated five-element phased-array cardiac coil and vector cardiographic triggering.
The free-breathing 2D approach consisted of a single-shot inversion-recovery SSFP delayed-enhancement MRI technique, with respiratory motion triggered using a respiratory belt, the authors explained.
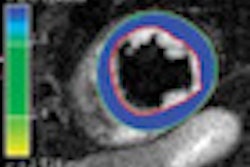
Infarct size was expressed as a percentage of the left ventricle, and the location and transmural extent of myocardial infarction were both assessed by visual score. The researchers evaluated the agreement between the 2D and 3D techniques using Bland-Altman analysis for infarct quantification, using kappa statistics to analyze the visual score.
The researchers found excellent agreement between the two techniques for infarct quantification (intraclass correlation = 0.99 [p < 0.01]; mean difference ± SD = 0.32% ± 2.4%).
For example, the mean value of the signal-to-noise ratio (SNR) of infarcted myocardium on the 2D inversion-recovery gradient-recalled echo (GRE) sequence was 22.0 ± 5.6 and 18.0 ± 4.4 for the 3D sequence. The mean SNR of infarcted myocardium was significantly higher for 2D (p = 0.029), while the mean SNR of normal myocardium was significantly higher for 3D (p < 0.005).
In addition, the contrast-to-noise ratio (CNR) of infarcted in relation to normal myocardium was not significantly different (p > 0.05), they noted. The mean CNR for 2D inversion-recovery GRE was 19.6 ± 9.1 and 15.7 ± 3.9 for the 3D technique.
Agreement for the transmural extent of infarction ranged from good to excellent between the free-breathing technique and the 3D breath-hold technique (kappa varied between 0.70 and 0.96 for all segments), and no regions of infarction were missed using the free-breathing approach.
However, total acquisition time was significantly shorter with the 3D technique (2.4 ± 0.9 minutes) compared to the 2D technique (4.9 ± 1.5 minutes) (p < 0.001).
"First, free-breathing, respiratory-triggered 2D single-shot inversion-recovery SSFP delayed-enhancement MRI is comparable to breath-hold 3D segmented gradient-echo inversion-recovery delayed-enhancement MRI when used for quantification of left ventricular scar," the authors wrote. "Second, the 2D technique with free breathing is well-tolerated and provides an alternative when patients are not capable of performing breath-holding. Third, CNR is higher for the 2D technique with free breathing compared with the 3D breath-hold technique."
On the other hand, 2D inversion-recovery fast low-angle shot imaging is the reference standard for assessing delayed hyperenhancement, requiring long acquisition times, and multiple breath-holds are needed to cover the entire left ventricle, they noted. In addition, 3D imaging in conjunction with a single, shorter breath-hold has been validated as a good way to overcome the limitations of the 2D technique.
The very similar visual scores for infarct location between the techniques indicate the potential clinical use of free-breathing acquisitions.
As for limitations, the 2D free-breathing technique was compared with the 3D breath-hold technique, but 2D inversion-recovery fast low-angle shot imaging with breath-holding is a more commonly used method.
"The excellent diagnostic value and clinical success rate of the 2D free-breathing technique support its clinical application as a possible first-line or second-line technique for assessing myocardial viability, depending on patient compliance and ability to follow breathing instructions," they concluded.
3D MRI at 3T speeds imaging
In the second study, Ludwig-Maximilian's Dr. Kerstin Bauner and colleagues examined the impact of 3-tesla MRI on reducing acquisition times.
Single-slice 2D MRI is used widely for myocardial viability imaging, usually in the form of an inversion-recovery GRE technique that detects MI and assesses viability. But imaging the entire left ventricle requires eight to 10 breath-holds of several heartbeats each. The use of 3D can shorten acquisition times, but potentially at a cost of CNR.
Imaging with 3-tesla MRI can potentially change the picture, making it easier on the patient, Bauner explained.
"Increased signal-to-noise ratio and CNR may be obtained ... when using the 3D inversion-recovery GRE sequence at 3T," they wrote. "Furthermore, the higher field strength offers the opportunity to increase spatial resolution. Therefore, a 3D inversion-recovery GRE sequence used at 3T might be a fast, alternative method for imaging myocardial viability with high spatial resolution" (AJR, June 2009, Vol. 192:6, pp. 1645-1650).
Their study compared a 3D inversion turbo fast low-angle shot (FLASH, 3D inversion-recovery GRE) sequence with a 2D inversion-recovery GRE sequence at 3 tesla for the noninvasive assessment of delayed enhancement in patients with chronic myocardial infarction.
The study examined 15 patients (10 men, five women, mean age 58 ± 8.9 years) with suspected MI. All images were acquired on a 3-tesla whole-body Magnetom Trio scanner with Total image matrix (Tim) coils (Siemens Healthcare, Erlangen, Germany) equipped with 32 independent receiver channels.
Bauner and colleagues performed a segmented breath-hold 3D inversion-recovery GRE technique with a voxel size of 6.3 mm3, compared to a breath-hold standard 2D inversion-recovery GRE technique with a voxel size of 21.3 mm3 for detecting delayed enhancement.
The group calculated CNR and measured infarct volumes. Detection and the transmural extent of infarctions were assessed using kappa statistics. Total acquisition times were measured for both sequences.
The results showed no significant differences in CNR between the 3D and 2D techniques. The correlation coefficients of the infarct volumes measured at 3D and 2D were r = 0.99 (p < 0.001). Similarly, calculations for the presence of hyperenhanced myocardium in all segments and the evaluation of transmurality yielded very good agreement (k = 0.98 and k = 0.90, respectively). However, total acquisition time was significantly shorter with the 3D technique (2.4 ± 0.9 minutes) than with the 2D technique (4.9 ± 1.5 minutes) (p < 0.001).
3D inversion-recovery GRE imaging at 3 tesla allows accurate assessment of myocardial infarction without loss of CNR compared with the standard 2D technique, and data acquisition time is significantly reduced, the authors concluded.
"The higher field strength at 3T compared with 1.5T results in several advantages," Bauner and colleagues wrote. "On the one hand, in theory the increased field strength of 3T yields a significantly higher SNR on contrast-enhanced T1-weighted sequences between infarcted and unenhanced normal myocardium compared with imaging at 1.5T. ... On the other hand, the benefit of the higher field strength may be equally pronounced when dealing with a higher temporal resolution or image acquisition in a fraction of time."
Another advantage of the higher spatial resolution is more accurate assessment of transmural extent of infarction of the myocardium, which may be a decisive factor in treatment, they wrote.
By Eric Barnes
AuntMinnie.com staff writer
June 15, 209
Related Reading
Heart groups update SPECT MPI guidelines, June 11, 2009
Cardiac magnetic resonance can assess at-risk myocardium after MI, June 5, 2009
3D CT detection of perfusion defects mirrors SPECT, March 8, 2009
Cardiac stress MR tops SPECT, showing cause of chest pain, November 30, 2008
Adenosine stress DECT equivalent to SPECT, MRI, November 21, 2008
Copyright © 2009 AuntMinnie.com