A new dual-source CT (DSCT) technique is able to distinguish between five types of kidney stones, offering the possibility of unprecedented detail in the noninvasive assessment of stone disease. The research could lead to improved management of patients with kidney stones.
The prospective phantom study from the Mayo Clinic in Rochester, MN, used supplementary beam filtering to increase separation of energy spectra and enable the differentiation of a "rainbow" of stone types, researchers said.
"Currently, in clinical practice, it is possible to differentiate uric acid stones from nonuric acid stones. However, there are so many different types of stones. Can CT differentiate among more stone types?" asked Mayo Clinic's Dr. Minliang Qu, who presented the results of the study at the 2009 RSNA meeting in Chicago.
The research was based on two key technologies, Qu said: First, dual-energy imaging using a dual-source CT scanner (Somatom Definition, Siemens Healthcare, Malvern, PA), and second, the use of additional beam filtering.
"When we plot the CT numbers [on the images], each individual stone type has a distinctive slope," Qu said. "The stone composition can be determined by its detected ratio: whether it's above or below the dissector of the two kidney stone types. The larger the dual-energy ratio difference, the better we can have the separation results."
The study examined 60 human renal stones (2 mm to 10 mm in diameter) of 10 different types:
- Uric acid (UA, n = 4)
- Uric acid dihydrate (UAD, n = 6)
- Ammonium acid urate (AAU, n = 6)
- Cystine (CYS, n = 6)
- Struvite (STR, n = 6)
- Calcium oxalate monohydrate (COM, n = 10)
- Calcium oxalate dihydrate (COD, n = 6)
- Carbonate apatite (CAP, n = 4)
- Brushite (BRU, n = 6)
- Hydroxyapatite (HA, n = 5)
The true stone composition was determined using micro CT and infrared spectroscopy. The stones were then embedded in porcine kidneys and placed into a 30-cm water phantom with a cadaver spine to test the DSCT method.
"We hypothesized that the dual-energy scanner can, first, increase the ratio difference between the uric and the nonuric acid, and, second, that we can differentiate more stone types and go beyond just uric acid and nonuric acid," Qu said in his presentation.
The two x-ray tubes of the DSCT scanner were set at 80 kV and 140 kV. Based on the differentiation of energies in Hounsfield units, the stone types could be separated into four different clusters.
The extra beam filter consisted of a 0.4-mm-thick tin filter added to the 140-kV tube of the DSCT scanner. Its purpose was to increase energy separation between the two spectra. Dual-energy CT (DECT) scans were acquired with and without the filter at 14 x 1.2-mm collimation for two phantom sizes: 30 and 35 cm.
Without the filter "there is significant [Hounsfield unit] overlap and only a small separation in spectra between the different materials," Qu said. "But using different separation [techniques] on different energy tubes, we were able to improve separation."
The first part of the study separated uric acid from the nonuric acid stones, Qu said, while the second part of the study separated the 60 stones into four groups.
Use of the tin filter permitted an increase in the dual-energy ratio for each materials group. Using DS-DECT with the extra filter on the 140-kV tube, 10 types of renal stones were able to be separated into the four groups, including:
- Group 1: uric acid, uric acid dihydrate, and ammonium acid urate (UA-UAD-AAU)
- Group 2: cystine and struvite (CYS-STR)
- Group 3: calcium oxalate monohydrate, dihydrate, and brushite (COM-COD-CAP-BRU)
- Group 4: hydroxyapatite, carbonate apatite (HA)
"This increased difference was most significant in the smaller phantom," Qu said. "The increase in the dual-energy ratio difference was 31% in the 35-cm phantom and 42% in the 30-cm phantom."
According to results in the 35-cm phantom, the dual-energy ratio difference increased from 0.31 without tin to 0.35 using the tin filter (10.4% increase) between the UA-UAD-AAU and CYS-STR groups. The dual-energy ratio increased from 0.12 to 0.23 (83.8% increase) between the CYS-STR and COM-COD-CAP-BRU groups. Finally, the dual-energy difference increased from 0.11 to 0.19 (67.7% increase) between the COM-COD-CAP-BRU and HA groups.
Use of additional beam filtration in DS-DECT increased measured differences in dual-energy ratio between stone types and allowed separation of 10 types of renal stones into four primary groups, Qu said, representing a significant improvement from the two-class discrimination technique (UA versus non-UA) that is currently possible without use of the tin filter.
The results are even better using the facility's new second-generation DSCT scanner (Somatom Definition Flash, Siemens) and a new software version, he said. The algorithm achieves the reliable separation of five types of stones, including cystine and struvite, which were previously lumped together. The five categories now include:
- Group 1: uric acid, uric acid dihydrate, and ammonium acid urate (UA-UAD-AAU)
- Group 2: cystine (CYS)
- Group 3 struvite (STR)
- Group 4: calcium oxalate monohydrate, dihydrate, and brushite (COM-COD-CAP-BRU)
- Group 5: hydroxyapatite, carbonate apatite (HA)
The ability to noninvasively discriminate more than simply uric acid versus nonuric acid renal stone types gives doctors better diagnostic and patient-management tools, Qu said.
 |
| Current DSCT techniques are capable of distinguishing between uric acid and nonuric acid stones. All images courtesy of Dr. Minliang Qu. |
 |
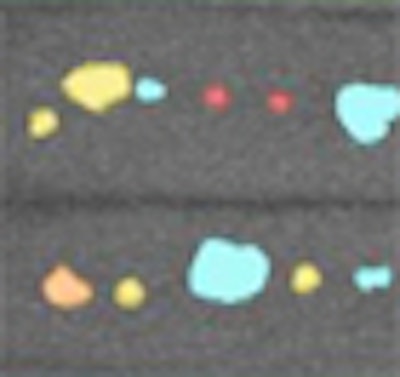
| Additional spectral filtering can successfully differentiate four (first-generation DSCT) or even five (second-generation DSCT) different stone types, including group 1: UA-UAD-AAU, group 2: CYS, group 3: STR, group 4: COM-COD-CAP-BRU, and group 5: HA. |
 |
| Continuum shows spectral relationship between different stone groups. |
"Using DECT with additional spectral filtration, we can first improve the separation ratio between uric acid and nonuric acid, and between these five groups," he said.
While certain stone types such as uric acid and small calcium stones are amenable to lithotripsy, other stone types such as cystine and brushite are very difficult to break up noninvasively and require surgical intervention, Qu said.
"If we can provide information noninvasively, we may be able to triage the patients," he said. "This could be especially important for patients with flank pain presenting to the emergency department," he said.
By Eric Barnes
AuntMinnie.com staff writer
January 4, 2010
Related Reading
Digital tomo works well for some kidney, ureteral stones, April 2, 2009
CT dose reductions don't impede detection of large renal calculi, March 18, 2009
DECT permits more detailed urinary stone analysis, December 4, 2008
Low-dose multidetector CT accurately evaluates urinary stone disease, March 30, 2007
Furosemide beats saline in MDCT urography, September 8, 2006
Copyright © 2010 AuntMinnie.com