VIENNA - The combination of 100-kV CT tube voltage and a low-noise reconstruction filter can significantly lower radiation dose in coronary CT angiography (CCTA) while maintaining image quality, according to a study presented at the European Congress of Radiology (ECR).
Researchers from the University of Pisa found that the low-voltage protocol cut radiation dose nearly in half. In addition, image quality of 2D and 3D reconstructions was comparable between the low-voltage protocol and standard reconstruction methods, according to presenter Dr. Lorenzo Faggioni. He presented the findings during a Thursday scientific session.
Over the past decade, the dramatic evolution of multislice CT technology has greatly improved the diagnostic performance of CT coronary angiography and broadened the spectrum of its clinical applications. However, these developments have also been paralleled by increasing radiation dose to patients, which can reach extremely high levels, Faggioni said.
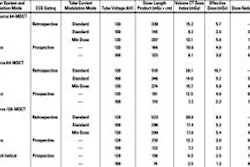
Strategies to reduce radiation dose in CCTA include online dose modulation, reduction of tube current, and reduction of tube voltage. Reduced tube voltage for CCTA of nonobese patients yields significantly increased contrast resolution with a lower radiation dose due to lower tissue penetration of x-rays generated and the maximization of photoelectric effects by iodine atoms of contrast media. However, lower voltage also increases image noise, Faggioni said.
To date, no data in the literature exist about the quality of 2D and 3D image reconstructions of coronary anatomy on low voltage CCTA, Faggioni said. As a result, the study team sought to evaluate the radiation dose of CCTA studies carried out using a tube voltage of 100 kV and a low-noise reconstruction filter, compared with a conventional tube voltage of 120 kV and a standard reconstruction kernel.
They also sought to assess the impact of the 100-kV acquisition technique on the diagnostic quality of 2D and 3D reconstructions performed with version 3.9 of the open-source OsiriX software.
Fifty nonobese patients, including 27 males and 23 females with comparable body mass index (BMI), received CCTA using the LightSpeed VCT (GE Healthcare) 64-detector-row CT scanner. For each CT dataset, one radiologist experienced in cardiac CT performed maximum intensity projection (MIP), curved planar reformation (CPR), and volume rendering (VR) reconstructions using the CMIV CTA software plug-in from Linkoping University in Sweden.
Panoramic MIP and volume rendered reconstructions of the coronary tree and CPR views of each coronary artery were generated. Two different radiologists then ranked the image quality of the studies in a blinded fashion using a three-point score (poor, good, or excellent).
The visual assessment found comparable image quality of the MIP, CPR, and VR views between both groups of datasets, Faggioni said.
Image quality ratings
|
A statistical trend was also seen toward better quality of CPR views on the 100-kV, low-noise filter protocol, he said.
At 9.8 ± 3.5 mSv, effective dose with the 100-kV protocol was significantly lower than the 18.3 ± 5.8 mSv produced by the 120-kV protocol (p < 0.0001). Despite the use of the low-noise kernel, however, image noise was significantly higher at 100 kV then at 120 kV, Faggioni said.
Faggioni acknowledged several limitations of the study, including the acquisition of all CCTA studies using retrospective ECG gating. Prospective ECG gating was unavailable at the time of the study and is very sensitive to arrhythmia, he said.
In addition, a very tight (70% to 80%) retrospective gating was used, but it still allowed for consistent dose reduction, he said. Also, patients with coronary stents or bypass grafts were excluded from the study.