Clinical history
The patient is a 12-year-old soccer player who injured himself while slowing to kick a ball. His lead foot slipped forward, causing him to fall with his lead leg flexed and his opposite leg extended. He experienced immediate pain in his right leg and hip.Physical exam and radiographic findings
The patient presented with acute pain and tenderness localized to the area of the buttock and upper thigh overlying the ischial tuberosity.
Plain radiographs, including an anteroposterior view of the pelvis, showed an avulsion of the right ischial tuberosity in the typical inferolateral location. An MR exam demonstrated osseous and soft-tissue edema, along with an avulsion fracture of the right ischial tuberosity (Figures 1-4).
Discussion
Avulsion fractures of the ischial tuberosity are most commonly seen in adolescents who engage in strenuous athletic competition. This is primarily due to the immaturity of the physis that has yet to undergo complete ossification. The muscle-tendon-bone unit of the hamstring muscles is subjected to significant stress during physical activity, and the physis serves as the weakest area and is thus prone to avulsion (British Journal of Sports Medicine online, June 22, 2007).
 |
| Figure 1. Anteroposterior conventional radiograph of the pelvis demonstrates an avulsion of a fragment of the inferolateral portion of the right ischial tuberosity (black arrows). |
In one large retrospective study, the most common avulsion injury of the pelvis involved the site of the ischial tuberosity, with gymnastics and soccer being the most common activities leading to this type of injury (Journal of Athletic Training, March 2001, Vol. 36:1, pp. 81-84).
 |
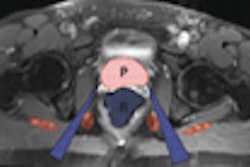
| Figure 2. Axial T2-weighted MR image of the pelvis shows increased signal within the soft tissue adjacent to the right ischial tuberosity (white arrows). |
This injury occurs with eccentric forceful movement of the hip toward flexion, while the knee remains at extension, placing strain upon the contracted hamstring muscles. Symptoms of an acute avulsion fracture of the ischial tuberosity may include pain in the buttock localized to the site of the ischial tuberosity, difficulty walking, standing, or squatting, and decreased range of motion in the thigh and lower leg (Journal of Bone and Joint Surgery, American volume, January 2007, Vol. 89:1, pp. 44-48; Journal of Athletic Training, March 2001, Vol. 36:1, pp. 81-84).
Symptoms are often indistinguishable from those of proximal hamstring muscle strain injuries, but a prompt and accurate diagnosis is essential to minimize the risk of complications, and determine if the injury is amendable to surgical repair or to conservative management.
Patients presenting with this type of injury may have pain in the thigh as well as overlying the ischial tuberosity. This nonlocalized pain distribution may lead to substantial delay in diagnosis of significant injury. If several weeks have elapsed since the injury, atrophy and weakness of the hamstring muscles may be noted (Skeletal Radiology, March 2001, Vol. 30:3, pp. 127-131).
 |
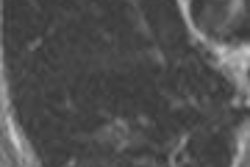
| Figure 3. Coronal T2-weighted MR image of the pelvis demonstrates increased signal intensity at the avulsion site on the right ischial tuberosity (black arrows). |
Conventional anteroposterior, axial, and oblique radiographs are often sufficient to confirm the diagnosis. CT, MRI, and ultrasonography may be used as adjuvant imaging to further delineate the extent of injury -- and the degree of soft-tissue involvement -- or to evaluate for fractures not visible by conventional radiographs (British Journal of Sports Medicine online, June 22, 2007).
Sciatic nerve injury has been reported following avulsion of the ischial tuberosity. Consequently, the clinician should be alert for pain and/or weakness in distribution of this nerve. The sciatic nerve may be damaged due to its proximity to the site of injury in the acute phase, or may be compressed from scar tissue formation that occurs chronically (Skeletal Radiology, March 2001, Vol. 30:3, pp. 127-131).
 |
|
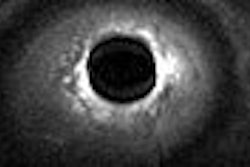
Figure 4. Coronal T1-weighted MR image optimally shows the fracture line between the ischial tuberosity fracture fragment and the remainder of the ischium (black arrows). All images courtesy of Adam D. Sharp and Dr. Douglas Beall.
|
Conservative treatment for avulsion injuries may include pain medications, rest, ice, heat, and gait improvement training. Additional exercises are often helpful to improve range of motion and strength. If significant improvement is not seen within four weeks after starting conservative therapy, surgical consultation should be sought to prevent such complications as nonunion, persistent weakness, pain, and decreased range of motion (Journal of Athletic Training, March 2001, Vol. 36:1, pp. 81-84).
Prompt surgical treatment has been recommended for avulsions with greater than 2.0 cm of inferior retraction, or for avulsions with sciatic nerve involvement (Archives of Orthopaedic and Trauma Surgery, 2000, Vol. 120:5-6, pp. 352-354).
Conclusion
Avulsion fractures of the ischial tuberosity are associated with forceful flexion of the hip (usually with the knee extended) and are most common among adolescent athletes, especially soccer players and gymnasts.
This injury is easily misdiagnosed due to similar presentation to other injuries involving the hamstrings. Conventional radiographs may be helpful to corroborate the diagnosis, and cross-sectional imaging may also be very helpful as in equivocal cases.
In addition to confirming the clinical diagnosis of this injury, cross-sectional imaging is of paramount importance in deciding between conservative therapy and surgery as the treatment of choice for the patient.
By Adam D. Sharp and Dr. Douglas P. BeallAuntMinnie.com contributing writers
August 10, 2007
Adam D. Sharp is a fourth-year medical student at the University of Oklahoma College of Medicine in Oklahoma City. He is pursuing a career in radiology.
Dr. Douglas Beall is the director of radiology services at Clinical Radiology of Oklahoma and an associate professor of orthopedics at the University of Oklahoma, both in Oklahoma City.
Related Reading
MR parameters divulge depth of acute hamstring injuries, July 13, 2007
MRI keeps pace with rapidly evolving musculoskeletal systems of young athletes, May 20, 2007
MRI, US take on diagnostic challenge of PAI in soccer players, August 18, 2006Copyright © 2007 AuntMinnie.com