
The microscopic intraductal component of breast cancer can cause local recurrence, even after breast conservation therapy. Unfortunately, this essential component is often missed during surgery. Clinicians in Japan tested ultrasound and MRI to see if they could detect intraductal invasive breast cancer and improve surgical accuracy.
For this retrospective study, Dr. Sangeetha Sundararajan and colleagues from the Institute of Clinical Medicine at the University of Tsukuba included 47 patients with 47 invasive breast cancers (27 with stage T1 cancer; 20 with stage T2). Other co-authors are from the Kyorin University School of Medicine in Kyorin.
The women underwent a sonographic exam, with a 12-5 MHz linear array transducer, which focused on detecting and measuring the extent of intraductal cancer (HDI 5000, Philips Medical Systems, Andover, MA). Some of the elements that the investigators looked for included solid duct dilatation radiation from the tumors and presence of satellite lesions.
MR exams were done on a 1.5-tesla scanner (Gyroscan NT Interna, Philips), and dynamic MR was performed in coronal planes using a 3D fast field-echo sequence. Imaging was done before and after contrast (10 mL of Gd-DTPA).
Ultrasound and MRI results were classified as true positive (TP) when an intraductal component wider than 15 mm was detected and confirmed by histopathology. Breast conservation surgery (2 x 4 lumpectomy) was followed by radiation therapy.
"If a wide intraductal component (> 15 mm) was diagnosed by US or MRI, wider resection, namely, quadrantectomy or modified radical mastectomy was performed," the authors explained (Radiation Medicine, March 2006, Vol. 24:2, pp. 108-114).
According to the results, histopathology revealed a wide intraductal component in 60% (28 of 47) of the patients. Of those 28, there were 16 TP and 19 true negative (TN) on sonography. Ultrasound underestimated intraductal disease for 12 false-negative cases (FN) and overestimated it (false positive or FP) in three patients. The modality's overall sensitivity was 57.1%, specificity was 84.2%, and accuracy was 68.1%.
 |
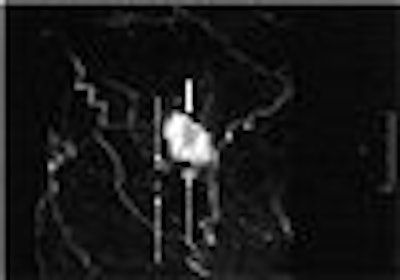
| Invasive ductal carcinoma in a 63-year-old woman. Above, ultrasound shows main tumor mass (white arrow) and satellite lesion (black arrow) with a ductal dilatation (dotted arrows) toward the nipple. The extent of intraductal component measured by ultrasound was 19 mm. Below, contrast-enhanced MRI study with maximum intensity projection (MIP) image shows main tumor (solid arrow) and satellite lesions (dotted arrows) in 3D coronal image. The extent of intraductal component measure by MRI was 18 mm. Histopathological studies diagnosed the invasive ductal carcinoma with satellite lesion and an intraductal component of 18 mm toward the nipple. |
 |
| Sundararajan S, Tohno E, Kamm H, Ueno Ei, Minami M, "Detection of Intraductal Component around Invasive Breast Cancer Using Ultrasound: Correlation with MRI and Histopathological Findings," Radiation Medicine, Vol. 24:2, pp. 108-114, 2006, Figure 2. |
MRI detected 14 TP cases out of 28 and 17 TN cases. MRI underestimated more cases than ultrasound (14 FN), but only overestimated disease in two patients. MR imaging's sensitivity was 50%, specificity was 89.5%, and accuracy was 65.9%.
In one case, neither MRI nor ultrasound detected intraductal cancer cells that were seen during surgery near the nipple area. In two patients, MRI found wide intraductal disease but underestimated the length by about 20 mm, the authors stated.
When combined, MRI and sonography yielded 75% sensitivity, 84.2% specificity, and 78.7% accuracy. While ultrasound alone showed a higher sensitivity than MRI, the ideal protocol for pinpointing intraductal disease would include both modalities, the authors concluded. By using the two tests together, disease underestimated was less likely and sensitivity was increased.
"Thus the surgeon more accurately could decide what type of surgery should be performed for the patient according to the presence or absence of wide intraductal extension of the tumor," they wrote.
The authors acknowledged that one limitation of the study was its retrospective design. But they added that they have performed a prospective study and are reviewing the results, which they believe will support their current conclusions.
By Shalmali Pal
AuntMinnie.com staff writer
May 1, 2006
Related Reading
Breast surgeon expresses reservations about screening US, April 13, 2006
Intraductal therapy effective in breast cancer model, March 8, 2006
Auto breast US handily spots lesions in early study, January 13, 2006
Lesion size, diameter, and location affect breast US interpretation, November 28, 2005
Copyright © 2006 AuntMinnie.com


















