For patients with suspected hypertrophic cardiomyopathy whose diagnoses aren't resolved by standard 2D echocardiography, cardiac MRI can successfully fill the diagnostic void, according to a new study.
Researchers from the Minneapolis Heart Institute Foundation in Minnesota, led by Dr. Carsten Rickers, published their findings in a recent journal issue from the American Heart Association (Circulation, August 9, 2005; Vol. 112:6, pp. 855-861).
The prospective study looked at 48 consecutive patients with established or suspected hypertrophic cardiomyopathy (HCM), all of whom were examined by 2D echo followed by same-day cardiac MRI (CMR).
While 2D echo is considered the gold standard noninvasive test for HCM, it has technical limitations, the authors noted. Specifically, the quantitative delineation of left ventricle (LV) wall thickness is dependent on adequate windows. In addition, cross-sectional images are often "unavoidably obtained with obliquity," the authors wrote, because the transducer is placed at a fixed point on the anterior chest wall.
Meanwhile, HCM is a heterogeneous disease that "appears in a myriad of diverse patterns, and with a wide range in the magnitude of wall thickening," the authors explained. "Although the distribution of hypertrophy is often diffuse, it is also frequently segmental and confined to relatively small regions of the LV chamber."
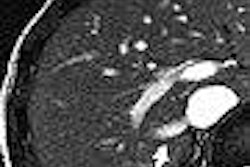
The practical effect of echo's limits in a diverse disease was that six of the 48 patients had "massive degrees" of hypertrophy, generally in the anterolateral free wall, that wasn't completely appreciated by echo but was by CMR.
"In this regard, the findings of the present study define a new subgroup of HCM patients and a novel diagnostic role for CMR imaging within the heterogeneous clinical and morphological spectrum of this disease," the authors wrote.
But CMR's identification of six additional patients who might be considered candidates for a preventive implantable defibrillator also creates a new clinical dilemma, the authors noted.
"To somehow extrapolate and translate the available echocardiographic data to CMR-derived wall thicknesses will require future prospective clinical studies with substantial follow-up spanning many years," they wrote.
"Therefore, at present, the most prudent strategy for such patients (with LV wall thickness ≥ 30 mm only by CMR) will require a measure of individual clinical judgment that relies on an integrated assessment of the overall sudden death risk profile to determine the advisability of recommending an implantable defibrillator," the authors wrote.
Some applications that may justify greater use of the more expensive modality may develop in the future, the authors speculated. "These include identification of the HCM phenotype when echocardiography is not of adequate diagnostic technical quality, as well as the recognition of delayed hyperenhancement after gadolinium infusion indicative of myocardial fibrosis," they wrote.
But even now, CMR should be considered for use in selected patients, the researchers stated.
"CMR imaging does not offer general superiority over echocardiography in all aspects regarding the morphological identification of the HCM disease phenotype, and at present, its use is not required in all HCM patients," the authors concluded. "Nevertheless, importantly, CMR is capable of establishing the diagnosis of HCM in some patients not reliably identifiable by conventional echocardiography."
By Tracie L. Thompson
AuntMinnie.com staff writer
August 26, 2005
Related Reading
Playing their hearts out: Do young athletes need cardiac screening? August 16, 2005
Family testing often reveals cause of sudden death, July 6, 2005
Echocardiography offers prognostic clues in peripartum cardiomyopathy, June 17, 2005
Imaging tackles cardiac 'octopus pot' syndrome, April 19, 2005
Cardiac magnetic resonance may spot unrecognized apical HCM, June 7, 2004
Copyright © 2005 AuntMinnie.com