MRI may hold the key to predicting fetal pulmonary hypoplasia, and improving chances of survival through early diagnosis. Japanese researchers have reported positive results with fetal lung measurements based on MR volume and signal intensity.
Fetal lung MR does not require fetal immobilization and produces clearer images with fewer motion artifacts, according to the multidisciplinary group from the Chiba University Hospital, Chiba University School of Medicine.
"MR imaging techniques allow detailed anatomic assessments, including estimation of lung volume, and can be used in place of (ultrasound)," wrote Dr Hisao Osada and colleagues. They did not consider conventional ultrasound because "the parameters are not sensitive or specific enough to be used in clinical decision making" (Radiology online, April 29, 2004).
"In this study, we demonstrated that fetuses with poor respiratory outcome after birth had significantly smaller lung volume between 24 and 39 weeks of gestation, compared with fetuses with good postnatal respiratory outcome," they wrote.
The findings are based on a sample size of 87 fetuses, of which 58 had good respiratory outcome (group A) and 29 had severe respiratory disturbance after birth (group B). All the fetuses were between 24-39 weeks of gestation.
The researchers performed planimetric measurement of total lung volume and calculation of the ratio of lung signal intensity to spinal fluid signal intensity (L/SF) on MR images using region-of-interest (ROI) analysis. Regression analysis, analysis of covariance, analysis of variance, and receiver operating characteristic (ROC) analysis were performed.
Imaging procedure
MR imaging was performed on a 1.5-tesla Signa system (GE Healthcare, Waukesha, WI) and a four-element phased-array surface coil. T1-weighted images were obtained with breath hold and a spoiled gradient-echo sequence. T2-weighted images were acquired in transverse, sagittal, and coronal planes with respect to the fetal thorax, using single-shot rapid acquisition and relaxation enhancement. The GE Advantage Windows RP (version 2.0) workstation was used for measuring each transverse section of a cross-sectional area of the lung.
 |
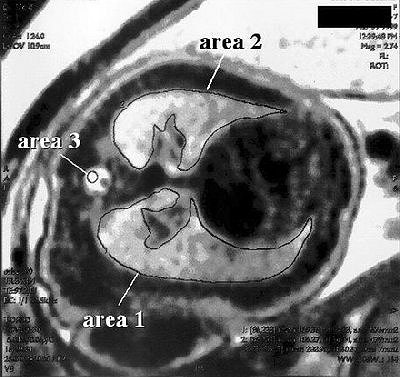
| Transverse MR image shows the process used to measure signal intensity of fetal lung and spinal fluid. The mean signal intensities (pixel value) in an ROI that covered the entire cross-sectional area of the right and left lungs (areas 1 and 2), and a circular ROI that covered the spinal canal (area 3), were measured in each transverse section. Figure 1 from Osada H, Kaku K, Masuda K, Itsuka Y, Seki K, Sekiya S. Quantitative and qualitative evaluations of fetal lung with MR Imaging. Radiology 2004; 231:887-892. |
To calculate the volume for each section, the value of the cross-sectional area was multiplied by that of the section thickness and intersection gap combined. The volumes of all of the sections were then summed to obtain the volume of the entire lung. The calculation was repeated for the other lung, and then the volumes of both lungs were added to obtain the total lung volume.
For calculating the L/SF using ROI analysis, the mean signal intensity of an ROI that covered the entire cross-sectional area of the right and left lungs on each transverse section was measured. Measurements from a circular ROI of spinal fluid were also obtained.
For each section, the mean signal intensity of the left and right lungs was divided by the signal intensity of the spinal fluid. This procedure was repeated for all lung sections, and the mean value for the L/SF ratio was obtained.
Statistical analyses were performed by using software (Statistical Package for the Social Sciences, version 10.5; SPSS, Chicago, IL). Regression analysis was used to evaluate for correlations between lung volume and gestational age or estimated fetal weight, and between L/SF ratio and gestational age or estimated fetal weight.
Results
The best fit for group A lung volume was represented by the regression line V = (2.41 x G) - 37.6 (r = 0.537, p < 0 .001) and that for group B, by V = (0.97 x G) - 14.0 (r = 0.378, p < 0.05) where V is the lung volume and G is the gestational weeks. Results of analysis of covariance with gestational weeks used as a covariate showed a significant difference in lung volume between the two groups (p < 0.001).
The mean ± SEM for L/SF ratio was 0.817 ± 0.013 and 0.598 ± 0.019 in groups A and B, respectively (P < 0.001). For prediction of postnatal respiratory outcome, the area under the ROC curve for lung volume and L/SF ratio combined was 0.990, significantly higher than that for lung volume alone (P < 0.05).
With the addition of planimetry, fetal volumetric measurements can readily be performed with MRI, the group concluded. MR volumetry can also be used in the evaluation of fetal pulmonary hypoplasia. Overall, the authors determined that "simultaneous use of volumetric and signal intensity measurements on MR images may play an important role in the evaluation of fetal pulmonary hypoplasia." They cautioned that further study was warranted, as there can be wide variability in the lung volume and L/SF ratio depending on gestational age.
By N. ShivapriyaAuntMinnie.com staff writer
May 27, 2004
Related Reading
Three-dimensional ultrasound shows utility in fetal lung volume measurements, March 18, 2004
Part II: The psychological impact of 3-D ultrasound on pregnant women, December 30, 2003
Part I: The psychological impact of 3-D ultrasound on pregnant women, December 29, 2003
MRI demonstrates fetal thymus, bronchial obstruction, May 12, 2003
Copyright © 2004 AuntMinnie.com