Radiologists in Essen, Germany, have designed a one-hour, whole-body MRI exam. It's not surprising, considering that these are the guys who built AngioSURF, the moving-table MR angiography system that offers a complete vascular assessment in 15 minutes. The relationship between the two exams is that AngioSURF 3D MRA, introduced in 2000, has been incorporated into the new whole-body MRI protocol.
At the 2002 European Congress of Radiology in Vienna, Dr. Thomas Lauenstein from the diagnostic radiology department of Essen's University Hospital discussed his preliminary results with whole-body MRI. The procedure is actually a multiorgan screening exam consisting of four protocols: cerebrovascular MRI, whole-body 3D MRA, cardiac MRI, and MR colonography. The scans, a sort of radiation-free version of whole-body CT, found unsuspected pathologies in unsuspecting volunteers.
Another presentation featured Dr. Mathias Goyen, AngioSURF developer and a principal of MR-Innovation, the spin-off firm that sells it. Goyen presented his latest whole-body MRA study in 100 patients with suspected peripheral artery disease. The two researchers communicated by telephone and e-mail with AuntMinnie.com, and their comments are included with the study results.
"In Europe it is generally forbidden by law to perform screening in conjunction with radiation exposure," Lauenstein said. "I think people in Europe are also more concerned about radiation than people in the U.S. This is certainly the strongest reason for us in Europe to focus on MRI (rather) than CT." Moreover, he said, MRI is noninvasive, has good patient acceptance, and high diagnostic accuracy.
Lauenstein, along with colleagues Dr. Christoph Herborn, Dr. Peter Hunold, Dr. Tobias Engelhorn, and Dr. Jörg Barkhausen, examined 38 subjects (aged 39-76, mean age 53.3 years). The subjects were considered healthy except for 11 with known hypertension and one with a prior colorectal polyp. None had contraindications for MRI, such as claustrophobia, metal implantation, or cardiac pacemakers.
The subjects underwent four MRI protocols on a 1.5-tesla Magnetom Sonata scanner (Siemens Medical Solutions, Erlangen, Germany) equipped with the AngioSURF rolling table platform and the following specifications: gradient strength of 40 mT/m; rise time, 200 msec; slew rate, 200 mT/m/ms; min TR/TE 1.5 ms/0.5 ms; chiller, 50 kW and 80 kVA. The researchers acquired four sets of images for each patient:
- Cerebrovascular MRI sequences included T1-weighted spin-echo, T2-weighted FLAIR (fluid-attenuated inversion recovery) and TOF (time-of-flight) using a head coil. No contrast was used, and total exam time was about 10 minutes.
- Whole-body MRA consisted of five contiguous 3D GRE acquisitions. Paramagnetic contrast (0.1 mmol per kg body weight Gd-BOPTA) (Multihance, Bracco Diagnostics, Milan, Italy) was administrated intravenously prior to MR angiography and for MR colonography.
- Cardiac MRI utilized late enhancement benefits of whole-body MRA contrast. The sequences consisted of TrueFISP cine (long and short axes) and IR (inversion-recovery) Turbo FLASH (fast low-angle shot). Total exam time was 20 minutes per patient.
- MR colonography consisted of a 3D VIBE sequence (75-second delay) following administration of a 2.5-liter water enema and administration of Gd-BOPTA per above. Images were then reconstructed into fly-through views, and examined for approximately 10 minutes.
According to the results, the mean examination time was 61 ± 6 minutes, and the exams were well tolerated by all patients. Perhaps more important, they resulted in the detection of 13 unsuspected pathologies, including 2 femoral artery stenoses, 1 renal artery stenosis, 2 cases of reduced myocardial ejection fraction, 2 cases of mitral regurgitation, 3 colorectal polyps, 1 cerebral aneurysm, and 2 aortic aneurysms.
 |
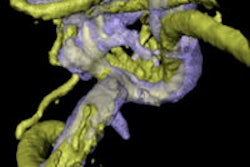
| Left, mitral-valve prolapse is discovered in a 57-year-old male patient during cardiac MRI portion of whole-body screening exam. Right, an unsuspected colorectal polyp is seen in a 49-year-old female patient during colorectal phase of whole-body screening. Images courtesy of Dr. Thomas Lauenstein. |
Discussion
Lauenstein said the study confirmed that rapid multi-organ screening with MRI is practical, and that it succeeded in identifying pathologies requiring subsequent follow-up. As for the high cost of the exam, Lauenstein said it was probably worth it.
"Unfortunately, the exam is quite expensive," he said. "But to calculate the real socioeconomic value of this project, a far higher number of patients have to be involved. Professor (Jörg) Debatin is planning to have this screening technique performed in 10,000 patients during the next 5 years. But even now we can tell that findings are certainly relevant for the patients that have (already) undergone screening."
Take the 3 colorectal polyps that were found. If these premalignant lesions had not been removed, they could easily have progressed to colorectal cancer in a couple of years, he said. Also, because MRI is still a "young" modality, its cost will certainly drop in coming years.
"What makes the whole procedure so attractive is that we can perform the (individual protocols) very quickly in a row," he said. "Imagine a person who wants to know about his health status (including brain, cardiac, vessels, bowel). Nowadays he has to go and see a neurologist, a cardiologist, a gastroenterologist, etc. This is very cumbersome. He needs 4 or 5 appointments (to) see 4 or 5 doctors.... We can provide the (patient's) health status in 60 minutes. Our patient only has to see one doctor, and only has to have one appointment. The entire procedure is noninvasive, and after 60 minutes, the patient can go back to work or whatever he feels like. So it is a big time savings."
The further adventures of AngioSURF
The idea of whole-body MR angiography makes perfect sense, according to Dr. Mathias Goyen, who like Lauenstein is a radiologist at University Hospital in Essen.
"Despite the early recognition that atherosclerotic disease is systemic in nature, the diagnostic approach has to date remained segmental," he said. "Generally, diagnostic assessment is limited to the particular vascular territory suspected of harboring arterial disease. Invasiveness, radiation exposure, contrast dose limitations, and cost represent the most critical hurdles preventing an all-encompassing approach to arterial imaging."
Whole-body MRA overcomes most of these limitations, he said. In a study of 100 patients using the AngioSURF (short for Angio system for Unlimited Rolling Fields of View) table and proprietary coil, the exam time of less than 15 minutes was only about 10% longer than single-station MRA.
The study by Goyen and colleagues sought to assess the potential of 3-D whole-body MRA to visualize additional atherosclerotic lesions in patients initially referred for MR assessment of peripheral vasculature.
One hundred patients (76 men, 24 women, mean age 62.4) were examined, all of whom had duplex ultrasound-documented peripheral artery disease, and 25 had conventional angiography.
Images were acquired using the 1.5-tesla Siemens Sonata scanner, equipped with high-performance gradients, which enabled a maximum amplitude of 40 mT/m and a slew rate of 200 mTm/s.
Based on a moving-vessel scout and following determination of the contrast travel time with a test bolus, slightly overlapping data sets were acquired using a FLASH 3D sequence (TR/TE 2.1/ 0.7 ms, flip angle 25°, 120-mm slab thickness, 64 interpolated 1.9-mm partitions, FOV of 380 x 380 mm, interpolated matrix of 512 x 512, and acquisition time of 12 seconds). A 2-cm overlap at each station’s end resulted in craniocaudal coverage of 174 cm. Achievable spatial resolution was 0.8 x 0.8 x 2 mm (post-interpolation pixel size) in the applied protocol, Goyen said.
A dose of 0.2 mmol/kg body weight of Multihance was administered intravenously in each patient using a biphasic injection scheme at 1.3 ml/sec (first flow rate) and 0.7 ml/sec (second flow rate).
According to the results, the exam provided diagnostic image quality from the carotid arteries to the tibial vessels, and was well tolerated in all patients. In addition to clinically suspected peripheral vascular disease, unsuspected findings were revealed in 23/100 (21%) of patients, including luminal narrowing in 50%. The findings included carotid artery stenosis (n=13), subclavian artery stenosis (n=2), aortic aneurysm (n=4) and renal artery stenosis (n=16). Patients received appropriate follow-up treatment where indicated.
Follow-up with single-station MRA or angioplasty was conducted in 26 patients at 60 days. Follow-up confirmed the diagnosis in 10 patients with carotid artery stenoses, 16 patients with renal artery stenoses, and 2 patients with subclavian artery stenosis.
For detection of significant stenosis, whole-body MRA had sensitivity of 95.3% and specificity of 95.2%. Concomitant disease, including abdominal aortic aneurysm (AAA), dissection, and bypass graft was correctly diagnosed in all cases, he said.
 |
| AngioSURF whole-body 3D MRA consists of five 3-D datasets acquired over 12 seconds each. Total acquisition time of 72 seconds includes 5 12-second acquisitions, with 3-second manual table repositioning between acquisitions. Total coverage is 180 cm from the supraaortic arteries to the runoff vessels. Above, whole-body MRA reveals an unsuspected infrarenal abdominal aortic aneurysm (maximum diameter 5.3 cm) in a 63-year-old male patient. Images courtesy of Dr. Mathias Goyen. |
Goyen also noted the limitations of the system. For example, intracerebral and coronary arteries are not well depicted. In some cases, AngioSURF's visualization of the infrapopliteal arteries is inadequate for presurgical planning. Digital subtraction of the precontrast images can often remedy this problem, but vascular surgeons often require focused single-station exams prior to surgery, he said. Finally, the coronary arteries are not well visualized using the AngioSURF protocol.
Goyen concluded that the system's most compelling strength is in screening. "Noninvasiveness, three-dimensionality, extended coverage, and high-contrast conspicuity are the characteristics of whole-body MRA using AngioSURF that combine to allow a quick, risk-free and comprehensive evaluation of the arterial system in patients with atherosclerosis," Goyen said. "The patients love it."
By Eric BarnesAuntMinnie.com staff writer
April 18, 2002
Related Reading
AngioSURF rides new wave in MR angiography, April 11, 2001
Copyright © 2002 AuntMinnie.com