Neuroimaging techniques should play a larger role in monitoring the effects of the human immunodeficiency virus (HIV) and in guiding therapy, according to a presenter at the 2003 International AIDS Society Conference on HIV Pathogenesis and Treatment in Paris.
But choosing the right imaging tools at the right time is vital, said Dr. Gabriele Arendt of the University of Dusseldorf in Germany during her talk. MRI, for instance, is best suited for patients in the late stages of disease, while PET and spectroscopy can yield information before clinical signs appear.
Arendt presented a long-term study of 743 out of 2,500 HIV-positive subjects who underwent MR exams. The scans revealed 206 lesions associated with opportunistic infections and 160 cases of HIV encephalitis. But 422 of the scans were completely normal, Arendt said, although the patients complained about neuropsychological deficits, including minor motor deficits (MMD).
"MRI is only a help if you’re looking for focal neurological signs in patients who are already showing clinical symptoms, such as paresis or ataxia," Arendt said in an interview with AuntMinnie.com.
Meanwhile, PET and MR spectroscopy (MRS) can help clinicians see how HIV patients are progressing on the neurological front before clinical signs appear, and may even give early warning signs that anti-retroviral therapy is failing.
Even when the virus appears to be fully controlled, it may be attacking brain cells, through a process that begins with an assault on the glial cells of the basal ganglia and the dopaminergic system, and later progresses to the neurons, Arendt explained.
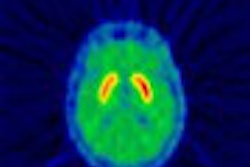
In another smaller study, her group used PET to study the cerebral glucose metabolism of 19 HIV-positive men who presented with MMD. Five had undetectable virus levels, and the rest had viral loads ranging from less than 1,000 to 30,000 copies of viral RNA per milliliter of blood.
"In patients responding to HAART (highly active antiretroviral therapy), we found an up-regulation of metabolism in the basal ganglia," Arendt said, while those who were either not on therapy, or failing therapy, showed a lowering of metabolism in the same region.
 |
| PET scan of an HIV-1 positive patient with decline of PET activity in the right basal ganglia (right side of the image). Image courtesy of Dr. Gabriele Arendt. |
Interestingly from a therapeutic point of view, the up-regulation appears to be an artifact of the viral attack; if the patients responded well to therapy, the metabolism returned to normal, she said.
"If the virus is stopped, the patient normalizes, the PET normalizes, the metabolism normalizes," Arendt said. "You know in which patients HAART is helping in the brain and in which it isn’t doing anything." This makes PET scanning a potentially useful tool for HIV-positive patients who seem to be responding to treatment based on conventional tests.
"If a patient has an active virus in the brain -- and not all patients will -- you know what the virus is doing to this individual patient," Arendt said. "What we should do is screen all patients with motor tests, and if we see pathological results, we put them into imaging."
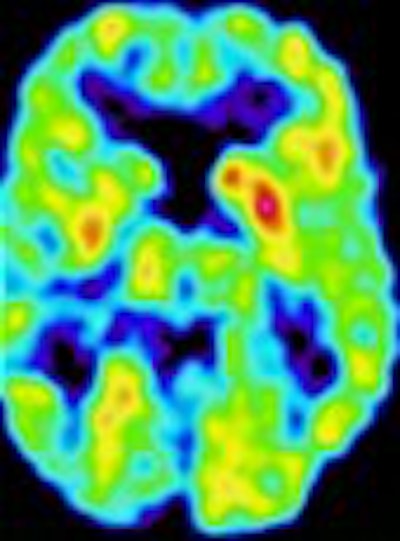
A third study -- testing 32 men with various levels of neurological symptoms -- showed that MRS can provide similar information about the stage of the HIV attack on brain cells, Arendt said.
 |
| MRS (glutamine/glutamate, myoinositol = mI, choline = Cho, creatine/phosphocreatine = Cr/PCr and N-acetylaspartate = NAA peaks) in an HIV-1 positive patient with a relative elevation of the myoinositol/creatine peak as a marker for glial proliferation. Image courtesy of Dr. Gabriele Arendt. |
In men with no symptoms, the tests showed no markers of cellular destruction; in those with minor symptoms, the glial cells appeared to be damaged, while in those with severe symptoms, there were signs of neuronal damage.
"This makes sense because the glial cells are the first to suffer damage and the neuronal cells are the last to die," she explained. The finding may have therapeutic implications, because a drug regimen may be most effective if it can halt a viral attack at the glial-cell stage, before the infection begins to destroy neurons.
"If you see neuronal damage, you can’t do anything," she said.
Finally, SPECT may also have a role in detailing which areas of the brain are most irritated by the virus. Arendt said that her clinic is experimenting with molecular imaging, in which radioactive tracers would be prepared that would bind to HIV viral proteins. Arendt’s group is currently synthesizing and testing the tracers, which could be ready for clinical testing in the near future.
"Then you would have centers in the brain lighting up when there is danger," she said. "This is my fantasy -- that you would put them in the scanner and if you got a red light, you would be able to say: ‘This brain is in danger.’ If we succeed in this, we will have done a big deal."
A report presented at the 2003 National HIV Prevention Conference in Atlanta earlier this month bolstered the importance of successful imaging strategies for HIV patients: Disease diagnoses among gay and bisexual men increased by 7.1% between 2001 and 2002, according to data from 25 U.S. states. This is the third annual increase reported for this population. Since the low point in 1999, HIV diagnoses among gay and bisexual men have risen by 17.7%, the reported stated.
By Michael SmithAuntMinnie.com contributing writer
August 7, 2003
Related Reading
Radiologists play important role in managing AIDS, July 2, 2002
Heart irregularities common in babies of HIV+ women, June 18, 2002
Abnormal chest x-ray may detect infection in patients with asymptomatic HIV disease, May 30, 2002
Neuroimaging warranted for patients with headache and advanced HIV infection, July 20, 2001
MR spectroscopy finds brain metabolite changes in asymptomatic HIV patients, November 22, 2000
Copyright © 2003 AuntMinnie.com