FDG has long shown its efficacy in demonstrating the metabolic differences between benign and malignant lung tumors. However, the radiotracer is not tumor-specific, and can render false-positive findings in tissue that is merely inflammatory. An alternative radiotracer for therapy response in the imaging of non-small cell lung cancer (NSCLC) may be fluorothymidine (FLT), a stable proliferation marker, German researchers have suggested.
FLT uptake correlates better with proliferation of lung tumors than does FDG uptake, according to Dr. Andreas Buck and colleagues. Buck is from the department of nuclear medicine at the University of Ulm in Germany; his co-authors are from the same institution, and represent the departments of thoracic surgery, pathology, and internal medicine.
"FLT turned out to be stable in vivo and accumulates in lung cancer cells in a proliferation-dependent manner," they wrote in the Journal of Nuclear Medicine (September 2003, Vol. 44:9, pp.1426-1431).
For their prospective study, the researchers examined 26 patients (17 men and 9 women) with a mean age of 62 years. The patients were selected when pulmonary nodules on CT scans suggested a malignant tumor. In 10 of the patients, core-biopsy specimens were used for histopathologic correlation; the remaining 16 had resective surgery within two weeks after their PET scans.
The FLT- and FDG-PET scans were performed on consecutive days within two weeks of either surgery or a core biopsy. The scans were performed on either an ECAT Exact or HR+ scanner (Siemens Medical Solutions, Erlangen, Germany), with an axial field of view of 15.5 cm per bed position. In all, five bed positions were measured for each patient, resulting in coverage of a total field of view of 77.5 cm.
An emission scan included the thorax and abdomen for all the patients, and the acquisition time was 10 minutes per bed position. All images from both FLT and FDG examinations were evaluated by two experienced nuclear medicine physicians.
"For calculation of standardized uptake value (SUV), circular regions of interest were drawn containing the area with focally increased pulmonary 18FFLT and 18FFDG uptake (lesional diameter at spiral CT, 4-48 mm)," the researchers wrote.
 |
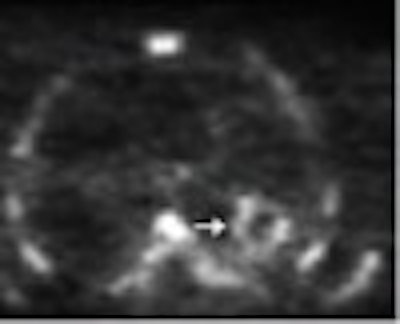
| Images from a patient with history of colorectal cancer and suggestive nodule in right middle lobe, for which histopathology revealed solitary tuberculoma. (A) Transaxial 18FFDG-PET scan demonstrates moderate 18FFDG uptake (arrow) in tumor. (B) No focal tracer accumulation is seen in corresponding 18FFLT-PET scan. (C) Corresponding CT scan shows pulmonary nodule in right middle lobe. (D) On Ki-67 immunohistochemistry, 5% of nuclei show immunoreactivity to Ki-67 antigen. Reprinted by permission of the Society of Nuclear Medicine from: Buck, A., et al. Imaging Proliferation in Lung Tumors with PET: 18FFLT Versus 18FFDG. J Nucl Med 2003, 44:1426-1431. |
In the FDG-PET studies, the mean SUV in the visible lesions was 4.1, and the mean maximum uptake was 6.9. In the 13 patients with NSCLC, the mean SUV was 5.6 and the mean maximum uptake was 9.7. The authors noted that four of the eight patients with benign lesions presented with focal FDG uptake.
For the FLT studies, the researchers reported a mean SUV of 1.8 in all visible lesions, and a mean maximum uptake of 2.7. In the NSCLC patients, FLT SUV was 3.2 and the mean maximum uptake was 4.7. They noted that no benign tumors showed local FLT uptake.
"Increased FLT uptake within a nodule was identified in 11 of the 13 patients with histologically confirmed NSCLC," they wrote.
The authors found a significant correlation between tumoral FLT uptake and proliferative activity as indicated by their Ki-67 immunostaining of malignant tissue specimens, with a mean correlation coefficient of 0.92 for FLT compared with a mean of 0.59 for FDG.
Although the authors found FLT to correlate significantly better with the proliferative activity of lung tumors, they cautioned that further studies with a larger patient population are needed to determine the diagnostic accuracy of the radiotracer. In addition, they emphasized that FDG-PET is more sensitive than FLT for staging disease in patients with malignant lung tumors.
"Because of three false-negative findings in our preliminary study, 18FFLT-PET may be less adequate than 18FFDG for primary staging in patients with known lung cancer, but may be more accurate for differentiation of unclear lung lesions," they wrote.
By Jonathan S. BatchelorAuntMinnie.com staff writer
October 1, 2003
Related Reading
PET detects lymph node activation during HIV infection, September 19, 2003
FDG-PET deemed most accurate for catching Hodgkin’s relapse, September 1, 2003
FDG shows promise as therapeutic agent for metastatic breast cancer, August 27, 2003
FDG-PET, scintigraphy offer a break in fever of unknown origin, August 22, 2003
PET imaging predicts response to chemotherapy for non-small cell lung cancer, August 4, 2003
Copyright © 2003 AuntMinnie.com


















