Flat-panel CT has a big advantage in the interventional suite, where it can potentially detect cerebral microbleeds without having to stop the procedure and send the patient to a conventional CT scanner.
But according to two new studies, flat-panel images still can't match those of conventional CT in sensitivity and specificity for detecting cerebral hemorrhage. Technical improvements, particularly higher image contrast, will be needed before the modality can compete on image quality. Considering the value of having a scanner where it's needed most, however, flat-panel CT should still be considered an option, researchers reported at the 2007 RSNA meeting in Chicago.
In one presentation, German researchers compared flat-panel CT to conventional cranial CT for detecting subarachnoid hemorrhage in phantoms. In another, a team from Austria examined the diagnostic value of flat-panel CT in the diagnosis of acute nontraumatic subarachnoid hemorrhage (SAH).
Versus conventional CT
Researchers from the University of Erlangen in Germany compared the resolution of flat-detector CT to conventional CT to "see what detectability could be provided" and evaluate local density changes with different sizes of brain bleeds, said Dr. Yiannis Kyriakou in his presentation.
The group compared the images generated on a conventional CT scanner (Somatom Definition, Siemens Healthcare, Erlangen, Germany) to those produced by a C-arm mounted flat-panel detector system (Axiom Artis 512² flat-panel detector with DynaCT software, Siemens).
Kyriakou and his team placed several tissue-equivalent spheres inside a head phantom to simulate different diameters (3, 5, 10, and 15 mm) of brain parenchyma bleedings. At conventional CT, the spheres had Hounsfield unit (HU) values of 0, 20, 30, 50 with respect to the surrounding water to simulate mixtures of blood and liquid, as well as pure blood. Each sphere was marked to distinguish it from the others.
"For the actual evaluation we compared detection rate profiles, which are defined as the (HU) values of the detected spheres of a certain contrast, and diameters (at flat-panel CT) compared to existing CT contrast and diameters," Kyriakou said.
The data were reconstructed using various slice thicknesses and kernels, and evaluated by two neuroradiologists and two medical physics experts in a double-blinded detection analysis. Visualization of each sphere was ranked on a five-point scale, with a 50% probability of detection used to define the limiting resolution of the system.
Flat-panel CT images show "we have some artifacts in the images which decreased detectability," Kyriakou said. "The comparison also shows that clinical CT performs better at the same dose level with respect to contrast levels."
Flat-detector CT provided generally lower contrast sensitivity compared to clinical CT. For an equivalent dose level (CTDIw = 4.0 mGy), a 5-mm lesion of 30 HU was detected at a slice thickness of 1 mm with the C-arm CT, while 5-mm lesion of 20 HU was detected at the same dose on a conventional CT scanner.
"At higher contrast levels of 30 HU or more, detectability will of course increase" Kyriakou said. Receiver operator characteristic (ROC) diagrams for both systems also showed the superiority of conventional CT.
Detecting SUH with flat-panel
In the next RSNA presentation, Dr. Stefan Celedin from LKH Klagenfurt (hospital) in Klagenfurt, Austria, discussed the diagnostic value of flat-panel CT for diagnosing acute nontraumatic subarachnoid hemorrhage (SAH).
"We have seen SAH in many patients with flat-panel CT, but it was a little bit disappointing because sensitivity and specificity were around or sometimes below 80%, so we found it's not equivalent to cranial CT," Celedin said. "In our opinion, technical improvements are still necessary. We couldn't prove it, but we still need the baseline CT. It's very helpful to have side-by-side reading to interpret flat-panel CT images more easily, and we found that flat-panel CT should be limited to the supratentorial region."
The group has spent two and a half years tinkering with its flat-panel CT scans, trying new techniques to improve image quality. For its part, Siemens has made improvements in its DynaCT software leading to reduced scaling and reconstruction times, Celedin said. In clinical use, patient positioning makes a difference, too. To reduce streaming artifacts, "tilt the head a little bit and get the teeth out of the way," he said.
The retrospective study examined data from 30 patients who presented to the emergency department with acute nontraumatic SAH verified by cranial CT. Following diagnosis of SAH, all patients underwent flat-panel CT scans of the head prior to angiography. The mean time interval between cranial CT and flat-panel CT was eight hours (0.5 to 17 hours).
First, blinded images were evaluated in a consensus reading two weeks prior to a side-by-side reading, Celedin said. The researchers compared multidetector-row CT images to flat-panel CT images for Claasen score, amount of supra- or infratentorial SAH, the visibility of ventricles, and the volume of eventual intracerebral hemorrhage.
In the blinded reading, Claasen scores of 1, 2, 3, 4, and 5 were seen in cranial CT and flat-panel CT in 0, 10%, 10%, 30%, and 50%, and 13%, 10%, 3%, 33%, and 40%, respectively, the researchers reported. Only 50% of the cases demonstrated agreement with the Claasen score.
Side-by-side reading of both sets of images increased total agreement to 66%. When looking at supratentorial SAH only, total agreement was found in 70%, with sensitivity of 87% and specificity of 86%. Side-by-side reading increased agreement to 83%, with sensitivity of 92% and specificity of 86% overall.
 |
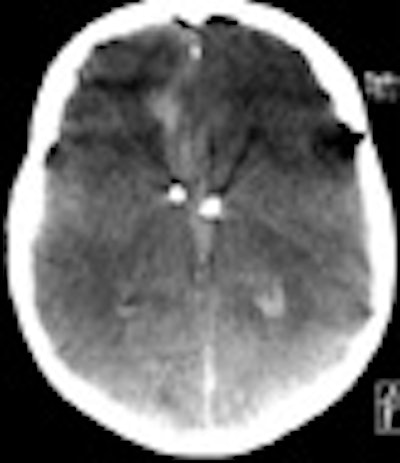
| A supratentorial subarachnoid hemorrhage (SAH) is missed at flat-panel CT (right). All images courtesy of Dr. Stephan Celedin. |
The infratentorial region showed total agreement in 50% of the cases. For detecting infratentorial SAH of any size, there were 13 false negatives, a sensitivity of 44% (23% to 66% CI), and a specificity of 86% (42% to 100% CI). For detecting infratentorial SAH 5 mm and larger, there were nine false negatives and two false positives, with sensitivity of 48% (23% to 72% CI) and specificity of 85% (55% to 98% CI).
Side-by-side reading improved agreement to 66% with a sensitivity of 61% and specificity of 100%. The temporal horn was not discernable with flat-panel CT in 7% of patients; the 4th ventricle could not be seen in half of the cases. Two intracerebral hemorrhages (50%) were missed at flat-panel CT, and two others were measured identically compared to cranial CT. In side-by-side viewing, a supratentorial intracerebral hemorrhage was detected.
 |
| Infratentorial subarachnoid hemorrhage (SAH) is missed at flat-panel CT. |
For visibility of any SAH in the supratentorial area, flat-panel CT yielded sensitivity of 88% (68%-97% CI Clopper-Pearson) and specificity of 83% (36% to 100% CI Clopper-Pearson), Celedin said. For detecting SAH 5 mm and larger, flat-panel CT yielded one false negative and five false positives, with sensitivity of 93% (68%-100% CI Clopper-Pearson) and specificity of 76% (38% to 88% CI Clopper-Pearson).
For detecting intraventricular blood, there were eight false negatives and three false positives at flat-panel CT, with sensitivity of 58% (33% to 80% CI) and specificity of 73% (39% to 94% CI), Celedin said.
The overall sensitivity of flat-panel CT was better for the supratentorial region compared to the infratentorial region, Celedin said, yet without reaching statistical significance (p = 0.272).
"When performing side-by-side reading, we did improve the overall results in most regions, especially in some subgroups, but this also didn't reach statistical significance," he said. "When it comes to cerebral hemorrhage, out of four we correctly diagnosed two with flat-panel CT."
Among the limitations of the study, the cohort was small, and there were no standardized window level settings for the reading.
"For almost every corner of the brain you have to search for the correct window setting to see what you want to see," he said. Also, considering the manufacturer's statement that a minimum 10-mm bleed can be detected using the flat-panel scanner, looking for smaller findings might not be germane, he said.
"Flat-panel CT can detect SAH with rather disappointing sensitivity and specificity," Celedin concluded. "We don't think it's equivalent to cranial CT, and technical improvements are necessary. Baseline CT images are helpful, and I think (flat-panel) should be limited to the supratentorial region, even though we could not prove it."
By Eric Barnes
AuntMinnie.com staff writer
February 1, 2008
Related Reading
Flat-panel detector CT bests MDCT in the skull base, March 7, 2006
Flat-panel detectors cut radiation dose in angiography, pediatric chest x-rays, November 4, 2005
Copyright © 2008 AuntMinnie.com
















