Kidney specialists may insist on calculating estimated glomerular filtration rates (eGFR) rather than serum creatinine (S-Cr) levels for assessing patients at risk of contrast-induced nephropathy (CIN). But the results of a six-year study from Virginia say one test is no better than the other for predicting renal failure.
The risks of contrast-induced nephropathy, a rare but serious complication following intravenous administration of iodinated contrast media, are known to be higher for patients with baseline renal dysfunction. For this reason, radiologists routinely look at serum creatinine (S-Cr) levels before performing contrast-enhanced CT scans.
But the relationship between S-Cr, eGFR, and renal failure is unclear, according to Dr. Amin Choudhri and colleagues from the University of Virginia Health Systems in Charlottesville.
"Predictor models exist to try to determine risks of contrast-induced nephropathy, but they're generally based on large doses of intra-arterial administration used in the cardiac literature," Choudhri said in a presentation at the 2007 RSNA meeting in Chicago, adding that limited data are derived from venous administration of IV contrast before CT. "To complicate things, the National Kidney Foundation has stated that estimated GFR is a more accurate assessment of renal function than serum creatinine (because) it attempts to normalize renal function for total muscle mass."
The study, based on an analysis of the institution's own clinical data repository from 2000 to 2006, aimed to determine the incidence of acute renal failure after administration of iodinated contrast, and determine whether eGFR is a more sensitive screening criterion than serum creatinine for predicting contrast-induced nephropathy.
The routine dose of iodinated contrast media was 100 cc of a low-osmolar contrast agent (range 100-150 cc) with a concentration of 350 mg/mL. Patients 14 years old and younger were excluded because weight-based dosing is used for children, Choudhri said.
Acute renal failure was defined as a rise in S-Cr of 0.5 mg/dL over baseline within three to five days after contrast-enhanced CT. eGFR was calculated using modification of diet in renal disease (MDRD) formula [eGFR (mL/min per 1.73 m²) = 186 x S-Cr-1.154 x age-0.203 x (0.742 if female) x (1.210 if black)].
"In all, 6,064 studies were found to meet the inclusion criteria, and in these studies 4.4% or 268 patients developed acute renal failure within three to five days after contrast-enhanced CT," Choudhri said. In line with previous studies, "the incidence of renal failure after CT was proportional to the baseline renal dysfunction," he said.
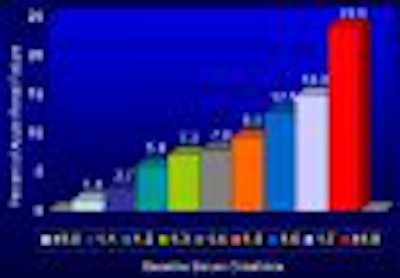
The results showed that the risk of renal failure increased steadily as S-Cr increased and eGFR decreased. "There was not a threshold that we identified -- (risk) seems to be continuous across the range, and similar results can be seen using baseline eGFR," Choudhri reported. "Those with the best renal function, eGFR greater than 90, had the lowest rate of renal failure at 1.2%. With decreases in eGFR, or more progressive renal failure, there are progressive increases in the degree of contrast-induced nephropathy. Interestingly, however, the patients with the lowest eGFR, 0 to 15, had a lower rate of acute renal failure than those with a moderate or severe decrease in baseline renal function."
There was no statistically significant difference between the two measures for predicting renal failure.
 |
| Prediction of renal failure based on S-Cr (above) and eGFR (below) revealed no statistically significant differences between the tests. All images courtesy of Dr. Amin Choudhri. |
 |
ROC analysis reflected very similar risk profiles, hence nearly identical curves for the two measures. S-Cr area under curve was 0.808, with a standard error 0.014 (95% CI, 0.779-0.836). For eGFR, the area under curve was 0.793, standard error 0.015 (95% CI, 0.764-0.823).
That curve showed that S-Cr of 1.4 mg/dL was approximately equivalent to eGFR of 46.5, "which is definitely more conservative than most people have been (estimating)," Choudhri said. An eGFR threshold of 60 mL/min (meaning an eGFR of 60 or higher can receive contrast, 59 and lower will not receive contrast) has similar statistical properties to an S-Cr threshold of 1.2 mL/dL, he said.
"Knowing the risks of contrast-induced nephropathy can aid in weighing the risks and benefits of contrast administration in patients with marginal renal function," Choudhri said. "In particular, contrast-enhanced CT may be the safest imaging modality for patients with baseline renal dysfunction or renal failure, especially considering what we know about gadolinium in patients with renal studies."
As for limitations, the study was retrospective and included both inpatients and outpatients at a single medical facility, Choudhri said. Owing to incomplete information, no adjustments were made regarding patients' comorbidities, use of dialysis, or any renal protective measures such as N-acetyl cysteine and bicarbonate that may have been used, though the results did compare only patients who had both S-Cr and eGFR tests before and after imaging. Finally, "there are other confounding factors and other cause of acute renal failure" in addition to the use of iodinated contrast, he said.
"The risk of acute renal failure after baseline contrast-enhanced CT is proportional to baseline renal dysfunction. eGFR and serum creatinine are equivalent in their ability to predict acute renal failure after the administration of iodinated contrast," Choudhri concluded.
An audience member said his own group's just-completed study yielded different results: In the subgroup of men older than 70 years, eGFR yielded 30% better detection of patients with nephropathy compared to S-Cr, the audience member said. Choudhri said his group's analysis showed no significant differences in any subgroup.
Lacking evidence that eGFR is better, why do nephrologists insist on using it? According to Choudhri, nephrologists' "long-term analyses of the risk of renal failures show that eGFR is more closely related to renal function," he said. "However, we do not have any evidence at this point that (eGFR) provides additional information for our purposes."
By Eric Barnes
AuntMinnie.com staff writer
December 18, 2007
Related Reading
Sodium bicarbonate best for prevention of contrast-induced nephropathy, October 29, 2007
MR experts take issue with FDA gadolinium warning, September 18, 2007
Trial shows promise for preventing radiocontrast nephropathy, December 7, 2006
Elderly need less contrast for pancreatobiliary imaging, August 2, 2006
Copyright © 2006 AuntMinnie.com

















