Belgian researchers are clearly catching up to the Italians in the art of prepless virtual colonoscopy, a technique that enhances patient comfort but adds work to the radiologist's day. In a modestly polyp-rich cohort, the Belgians achieved 100% sensitivity for lesions 10 mm and larger, using optical colonoscopy as their reference standard.
At the 2006 International Symposium on Virtual Colonoscopy in Boston, Dr. Didier Bielen from University Hospital Gasthuisberg at the Catholic University of Leuven in Belgium, presented results from the first 75 patients to undergo prepless virtual colonoscopy followed by a same-day cathartic prep and optical colonoscopy.
The aim of the VC tagging-only prep study was to assess "the feasibility of the technique and document its performance," Bielen said.
The 75 men and women in the study (mean age 44, range 60-73) had "mainly nonhigh-risk suspicions" of colonic pathology "without a family or personal history of colorectal cancer or advanced adenomas," he said. In about half of the patients that meant a positive fecal occult blood test (FOBT).
Of the 60 patients (30 men, 30 women) whose exams were completed in time for the abstract, 32 had a positive FOBT. As for the rest, 26 of the 60 had a personal history of CRC or advanced adenoma, 2 had a family history of advanced neoplasia or colorectal cancer, according to the abstract.
Two days prior to imaging, Bielen and his colleagues Ingrid Demedts, Ph.D., and Guy Marchal, Ph.D., put the 75 subjects on a nonstandardized low-fiber diet. Tagging was achieved with a 100 mL dose of water-soluble iodinated contrast (meglumine ioxitalamate 3%, Telebrix Gastro Guerbet/Codali, Brussels, Belgium), which has a mild cathartic effect.
"The tagging agent was given one day prior to the exam with meals," Bielen said. The patients consumed a dose with the daytime and evening meals, and "the remaining 20 mL were added the morning of the exam."
All images were acquired on a 16-detector-row CT scanner (Somatom Sensation 16, Siemens Medical Solutions, Erlangen Germany) using 16 x 1.5-mm or 16 x 0.75-mm collimation, 15 mAs, and 2-mm slice thickness.
Fifty-one exams were performed using 2D CareDose (Siemens) dose modulation, and the remaining 24 exams with CareDose 4D, which allows for additional dose modulation along the z-axis. The images were evaluated on a PACS workstation for the primary 2D viewing and a dedicated 3D workstation (syngo Colonography, Siemens) for 3D confirmation and problem-solving, according to Bielen. Insufflation was performed using CO2 gas.
After the VC exam, all patients underwent cathartic cleansing with 4-5 L of an electrolyte solution followed by same-day optical colonoscopy, which served as a reference standard. To compare the results of the two exams, colonoscopy results were segmentally unblinded using a technique described by Pickhardt et al (New England Journal of Medicine, December 4, 2003, Vol. 349:23, pp. 2191-2200).
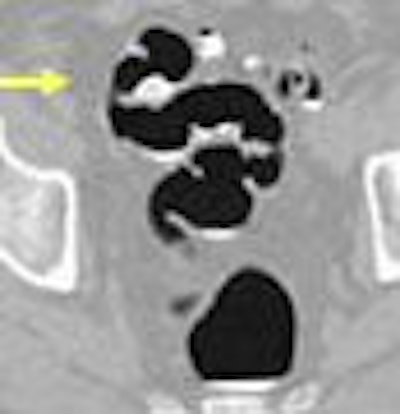
The imaging results showed "residual fluid covering less than 20% of the colonic surface," Bielen said. "This fluid was homogeneously tagged in the majority of patients: 72 of 75. Nine patients showed a high-density film covering parts of the colonic surface," he said. "Two patients showed rather inhomogeneously tagged fluid with a lower density of around 200 HU -- this was especially true in the right side of the colon."
 |
| Residual fluid covered less than 20% of the colonic surface, and with prone and supine scanning, did not impair radiologists' ability to interpret data. Images courtesy of Dr. Didier Bielen. |
Residual stool was present in varying amounts in most patients, and stool tagging was homogeneous in just two patients, Bielen said. Even so, the inhomogeneously tagged stool was relatively easy to distinguish from lesions by its texture, and as it changed position between supine and prone scanning.
 |
| Stool tagging was less successful than fluid tagging, yielding homogeneous tagging results in only two patients. As a result, extra time was needed to distinguish this stool from colonic polyps and mucosa. Images courtesy of Dr. Didier Bielen. |
The combined VC and colonoscopy results were normal in 32 of 75 patients, and lesions 5 mm and smaller were found in 30 patients (VC detected 11/95). Four patients had polyps 6-7-mm in diameter (VC detected 3/8), two patients had polyps 8-9-mm in diameter (VC detected 4/5), six had polyps 10-mm or larger (VC detected 7/7), and one patient had a rectosigmoid tumor, also seen in both exams.
 |
| A sigmoid tumor, 5 x 2 cm in size, was detected at both VC and colonoscopy. The lesion was a well- to moderately differentiated transmural invasive adenocarcinoma classified as pT3N2Mx R0. Images courtesy of Dr. Didier Bielen. |
For lesions 8 mm and larger, VC's specificity and sensitivity (positive and negative predictive values) were 91% and 99%, respectively, Bielen said, and 100% for lesions 10 mm and larger.
 |
| The results showed high sensitivity, specificity, and negative predictive value for tagged prepless virtual colonoscopy, particularly among lesions 8 mm or larger in diameter. Chart courtesy of Dr. Didier Bielen. |
A previous study by Iannacone et al from the University of Rome in Italy yielded 92% sensitivity for polyps 8 mm or larger for prepless VC in an average-risk cohort of 180 patients.
"We conclude that (VC) using water soluble tagging agents is feasible in daily practice," Bielen said. "It gives you acceptable tagging for residual fluid, but poses a problem for residual stool. Nonetheless promising results (showed) high specificity and sensitivity and negative predictive values, especially for lesions above 8 mm."
In response to a question from the audience, Bielen said interpretation times are slightly longer than for regular VC with a cathartic prep, mostly due to the extra time needed to assess inhomogeneously tagged stool. Primary 2D viewing is required for prepless VC, with 3D used for confirmation and problem-solving, he said. On the other hand, first-pass 3D endoscopic interpretation would be impractical and time-consuming, he said, producing a lot of "bumps" that would need to be evaluated individually in 2D.
By Eric Barnes
AuntMinnie.com staff writer
December 6, 2006
Related Reading
Prepless VC misses some diminutive flat lesions, November 17, 2006
Reduced prep, low-residue diet, and mild tagging suffice for accurate VC, July 13, 2005
Prepless VC yields high sensitivity in average-risk subjects, June 10, 2005
Iodine tagging regimen yields best VC results, January 27, 2005
Copyright © 2006 AuntMinnie.com

















